

Effect of Alteplase vs Aspirin on Functional Outcome for Patients With Acute Ischemic Stroke and Minor Nondisabling Neurologic Deficits: The PRISMS Randomized Clinical Trial
- PMID: 29998337
- PMCID: PMC6583516
- DOI: 10.1001/jama.2018.8496
Effect of Alteplase vs Aspirin on Functional Outcome for Patients With Acute Ischemic Stroke and Minor Nondisabling Neurologic Deficits: The PRISMS Randomized Clinical Trial
Abstract
Importance: More than half of patients with acute ischemic stroke have minor neurologic deficits (National Institutes of Health Stroke Scale [NIHSS] score of 0-5) at presentation. Although prior major trials of alteplase included patients with low NIHSS scores, few without clearly disabling deficits were enrolled.
Objective: To evaluate the efficacy and safety of alteplase in patients with NIHSS scores of 0 to 5 whose deficits are not clearly disabling.
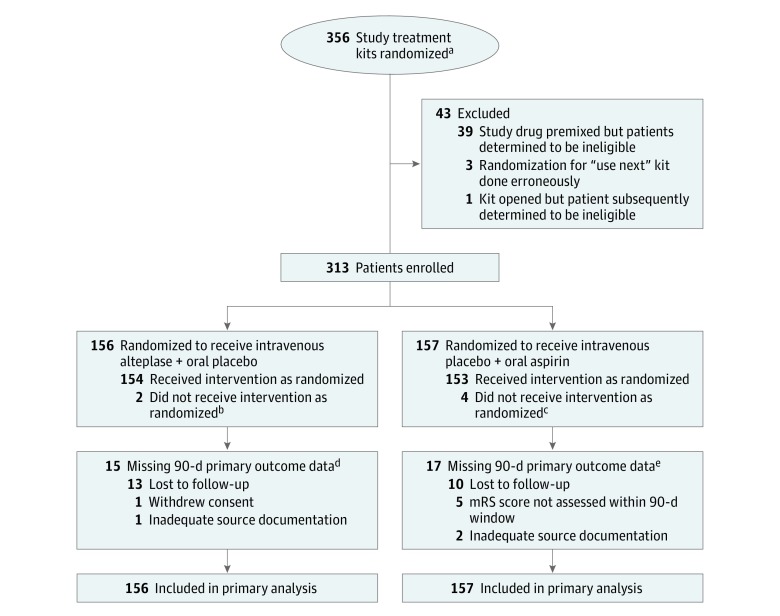
Design, setting, and participants: The PRISMS trial was designed as a 948-patient, phase 3b, double-blind, double-placebo, multicenter randomized clinical trial of alteplase compared with aspirin for emergent stroke at 75 stroke hospital networks in the United States. Patients with acute ischemic stroke whose deficits were scored as 0 to 5 on the NIHSS and judged not clearly disabling and in whom study treatment could be initiated within 3 hours of onset were eligible and enrolled from May 30, 2014, to December 20, 2016, with final follow-up on March 22, 2017.
Interventions: Participants were randomized to receive intravenous alteplase at the standard dose (0.9 mg/kg) with oral placebo (n = 156) or oral aspirin, 325 mg, with intravenous placebo (n = 157).
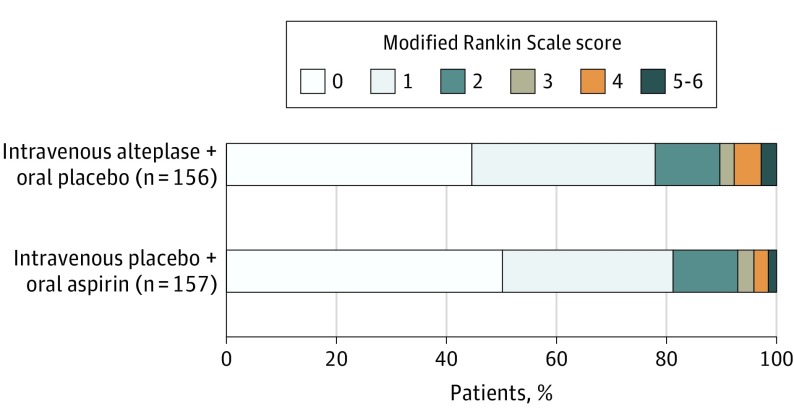
Main outcomes and measures: The primary outcome was the difference in favorable functional outcome, defined as a modified Rankin Scale score of 0 or 1 at 90 days via Cochran-Mantel-Haenszel test stratified by pretreatment NIHSS score, age, and time from onset to treatment. Because of early termination of the trial, prior to unblinding or interim analyses, the plan was revised to examine the risk difference of the primary outcome by a linear model adjusted for the same factors. The primary safety end point was symptomatic intracranial hemorrhage (sICH) within 36 hours of intravenous study treatment.
Results: Among 313 patients enrolled at 53 stroke networks (mean age, 62 [SD, 13] years; 144 [46%] women; median NIHSS score, 2 [interquartile range {IQR}, 1-3]; median time to treatment, 2.7 hours [IQR, 2.1-2.9]), 281 (89.8%) completed the trial. At 90 days, 122 patients (78.2%) in the alteplase group vs 128 (81.5%) in the aspirin group achieved a favorable outcome (adjusted risk difference, -1.1%; 95% CI, -9.4% to 7.3%). Five alteplase-treated patients (3.2%) vs 0 aspirin-treated patients had sICH (risk difference, 3.3%; 95% CI, 0.8%-7.4%).
Conclusions and relevance: Among patients with minor nondisabling acute ischemic stroke, treatment with alteplase vs aspirin did not increase the likelihood of favorable functional outcome at 90 days. However, the very early study termination precludes any definitive conclusions, and additional research may be warranted.
Trial registration: ClinicalTrials.gov Identifier: NCT02072226.
Conflict of interest statement
Figures
Comment in
-
Intravenous Alteplase for Mild Nondisabling Acute Ischemic Stroke: A Bridge Too Far?JAMA. 2018 Jul 10;320(2):141-143. doi: 10.1001/jama.2018.8511. JAMA. 2018. PMID: 29998321 No abstract available.
-
Primary stroke centers: are they worthy of an upgrade?Intern Emerg Med. 2019 Mar;14(2):333-334. doi: 10.1007/s11739-018-1999-3. Epub 2018 Dec 12. Intern Emerg Med. 2019. PMID: 30542821 No abstract available.
References
-
- Schwamm LH, Ali SF, Reeves MJ, et al. . Temporal trends in patient characteristics and treatment with intravenous thrombolysis among acute ischemic stroke patients at Get With The Guidelines–Stroke hospitals. Circ Cardiovasc Qual Outcomes. 2013;6(5):543-549. doi:10.1161/CIRCOUTCOMES.111.000095 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
