

Effect of extra-amniotic Foley's catheter and vaginal misoprostol versus vaginal misoprostol alone on cervical ripening and induction of labor in Kenya, a randomized controlled trial
- PMID: 30001195
- PMCID: PMC6044072
- DOI: 10.1186/s12884-018-1793-2
Effect of extra-amniotic Foley's catheter and vaginal misoprostol versus vaginal misoprostol alone on cervical ripening and induction of labor in Kenya, a randomized controlled trial
Abstract
Background: The safest, most effective and fastest combined approaches to induction of labor is unknown. In an open-label randomized clinical trial we evaluated the efficacy of combination of extra-amniotic Foley's catheter and vaginal misoprostol compared to vaginal misoprostol alone for cervical ripening and induction of labor on the incidence of failed induction, induction-to-delivery interval and adverse maternal and perinatal outcomes.
Methods: Pregnant women at gestational age of 28 weeks or greater admitted at Kenyatta National Hospital, Kenya for induction of labor were enrolled then randomized to either a combination of extra-amniotic Foley's catheter inflated by 30 cm3 of normal saline and 25 micrograms of vaginal misoprostol or 25 micrograms of vaginal misoprostol alone. Women underwent 6 hourly reviews and additional misoprostol inserted if required. The primary outcome was incidence of failed induction. Secondary outcomes were induction-to-delivery interval and adverse maternal and perinatal outcomes. We conducted an intent-to-treat analysis and compared means or medians using t-test or Wilcoxon rank, proportions using Chi-square or Fishers test as appropriate. Induction-to-delivery interval were compared using the log-rank test. P-values of < 0.05 and 95% confidence intervals that excluded the null were considered statistically significant.
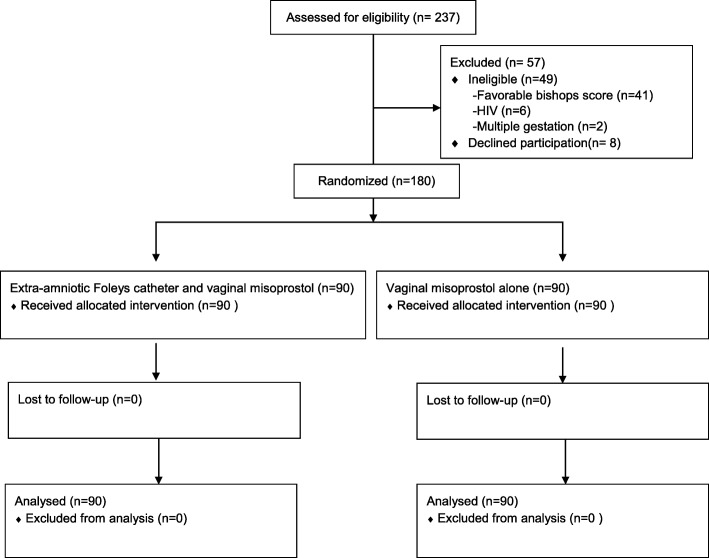
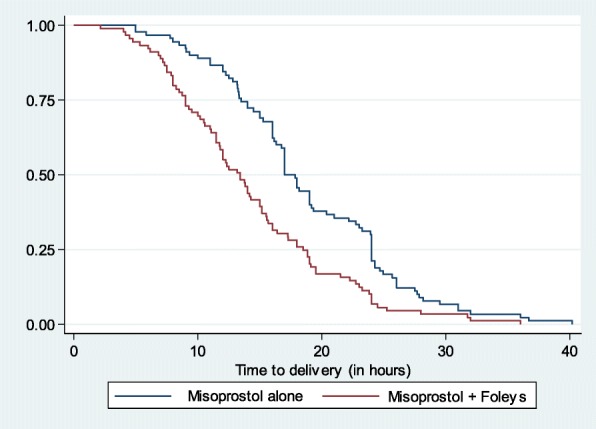
Results: Between February and May 2016, we enrolled 180 of 237 pregnant women admitted for induction of labor and randomized them to either a combination of extra-amniotic Foley's catheter and vaginal misoprostol (n = 90) or vaginal misoprostol alone (n = 90). The socio-demographic and obstetric characteristics were similar between the two groups. Failed induction rates were lower but not statistically significant following combined extra-amniotic Foley's catheter and vaginal misoprostol (8.9%) versus vaginal misoprostol alone (11.1%). The mean induction-to-delivery time was 4.8 h shorter in the combined extra-amniotic Foley's catheter and vaginal misoprostol (mean 18.9, standard deviation (SD) 7.2 h) compared to misoprostol only group (mean 14.1, SD 6.9 h) (log-rank test, p < 0.001). Maternal and perinatal complications were similar between the two groups.
Conclusions: Extra-amniotic Foley's catheter and vaginal misoprostol for cervical ripening and induction of labor did not significantly lower the incidence of failed induction but safely shortened induction-to-delivery time compared to vaginal misoprostol only.
Trial registration: Trial was retrospectively registered on 14-03-2016 PACTR201604001535825.
Keywords: Failed induction; Foley’s; Induction-to-delivery; Misoprostol; RCT.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval was obtained from Kenyatta National Hospital/University of Nairobi Ethical Research Committee (P71/02/2015). Written informed consent was obtained from all research participants. The informed consent process and form was approved by the ethics committee.
Competing interests
The authors declare no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Managing complication in pregnancy and childbirth: a guide for midwives and doctors. Geneva, World Health Organization, 2000 http://www.who.int/maternal_child_adolescent/documents/managing-complica.... Accessed 25 Feb 2018.
-
- WHO recommendations for induction of labor. http://apps.who.int/rhl/pregnancy_childbirth/induction/guidelines_goonew.... Accessed 25 Feb 2018.
-
- Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, Kirmeyer S, et al. Births: final data for 2006. Natl Vital Stat Rep. 2009;57:1–102. - PubMed
-
- ACOG Practice Bulletin No. 107: Induction of labor. ACOG Committee on Practice Bulletins -- Obstetrics. Obstet Gynecol. 2009;114(2 Pt 1):386–97. 10.1097/AOG.0b013e3181b48ef5. - PubMed
-
- Esiromo A.M. Outcomes of pharmacological induction of labour at or near term at Kenyatta National Hospital http://obsgyn.uonbi.ac.ke/sites/default/files/chs/medschool/obsgyn/DR.%2.... Accessed 25 Feb 2018].
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
