

Application of 3D Fast Spin-Echo T1 Black-Blood Imaging in the Diagnosis and Prognostic Prediction of Patients with Leptomeningeal Carcinomatosis
- PMID: 30002052
- PMCID: PMC7410554
- DOI: 10.3174/ajnr.A5721
Application of 3D Fast Spin-Echo T1 Black-Blood Imaging in the Diagnosis and Prognostic Prediction of Patients with Leptomeningeal Carcinomatosis
Abstract
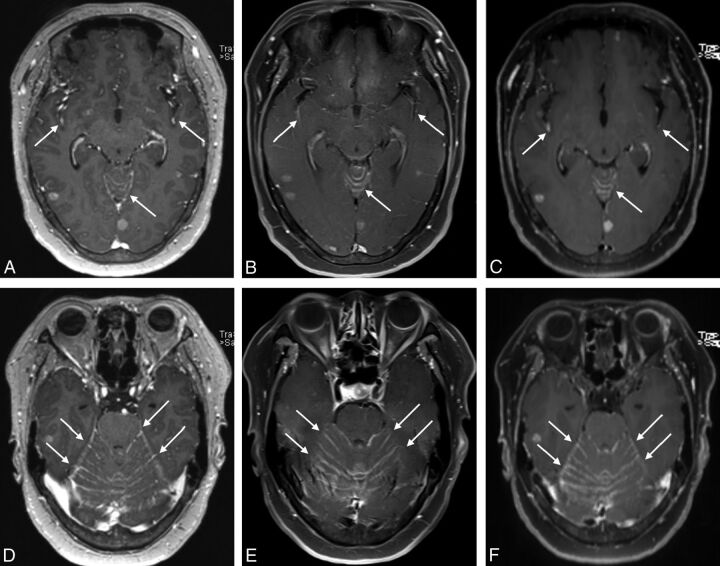
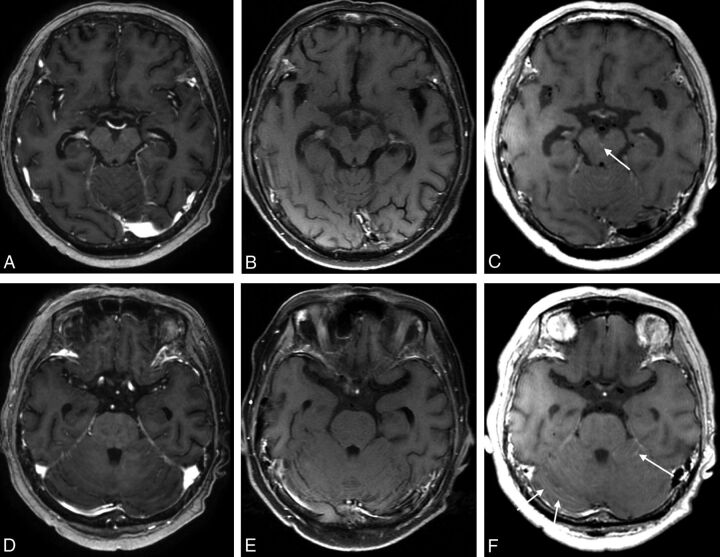
Background and purpose: Contrast-enhanced 3D fast spin-echo T1 black-blood imaging selectively suppresses the signal of blood flow and could provide a higher contrast-to-noise ratio compared with contrast-enhanced 3D ultrafast gradient recalled echo (contrast-enhanced gradient recalled echo) and 2D spin-echo T1WI (contrast-enhanced spin-echo). The purpose of our study was to evaluate whether black-blood imaging can improve the diagnostic accuracy for leptomeningeal carcinomatosis compared with contrast-enhanced gradient recalled-echo and contrast-enhanced spin-echo and, furthermore, to determine whether the grade of leptomeningeal carcinomatosis evaluated on black-blood imaging is a significant predictor of progression-free survival.
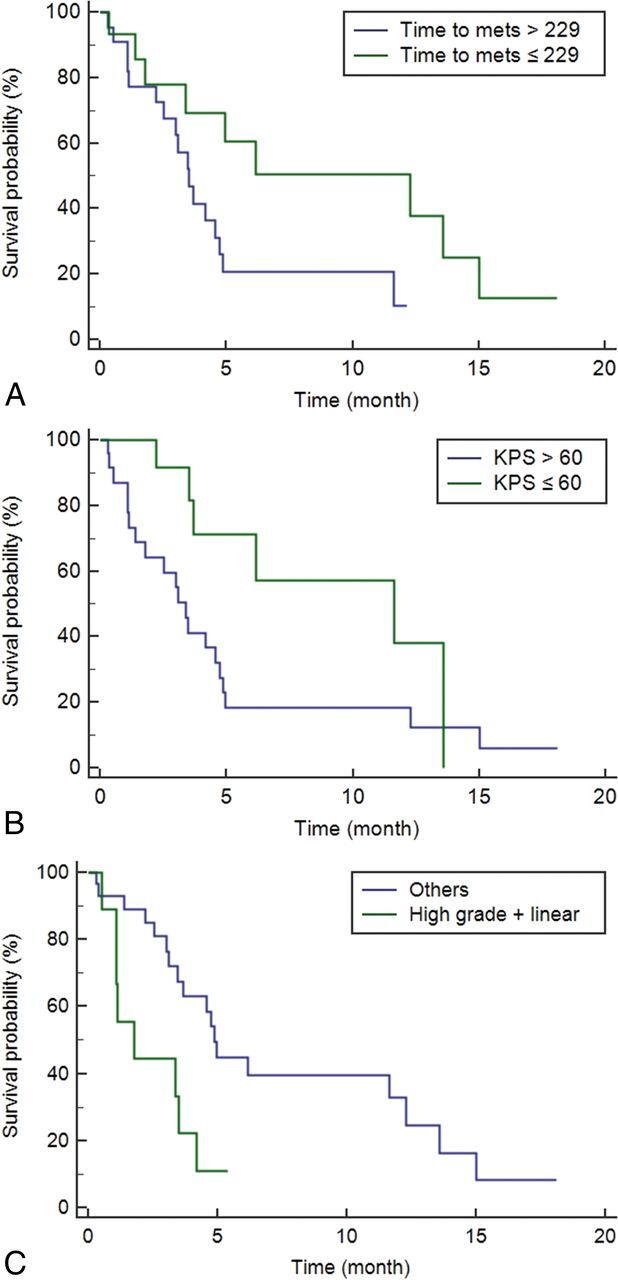
Materials and methods: Leptomeningeal carcinomatosis (n = 78) and healthy (n = 31) groups were enrolled. Contrast-enhanced gradient recalled-echo, contrast-enhanced spin-echo, and black-blood imaging were separately reviewed, and a diagnostic rating (positive, indeterminate, or negative) and grading of leptomeningeal carcinomatosis were assigned. The diagnostic accuracies of the 3 imaging sequences were compared in terms of leptomeningeal carcinomatosis detection. The Kaplan-Meier and the Cox proportional hazards model analyses were performed to determine the relationship between the leptomeningeal carcinomatosis grade evaluated on black-blood imaging and progression-free survival.
Results: Black-blood imaging showed a significantly higher sensitivity (97.43%) than contrast-enhanced gradient recalled-echo (64.1%) and contrast-enhanced spin-echo (66.67%) (P < .05). In terms of specificities, we did not find any significant differences among contrast-enhanced gradient recalled-echo (90.32%), contrast-enhanced spin-echo (90.32%), and black-blood imaging (96.77%) (P > .05). A Cox proportional hazards model identified the time to metastasis, Karnofsky Performance Scale status, and a combination of the leptomeningeal carcinomatosis grade with a linear pattern as independent predictors of progression-free survival (P < .05).
Conclusions: Black-blood imaging can improve the diagnostic accuracy and predict progression-free survival in patients with leptomeningeal carcinomatosis.
© 2018 by American Journal of Neuroradiology.
Figures
Comment in
-
Reply.AJNR Am J Neuroradiol. 2018 Dec;39(12):E126. doi: 10.3174/ajnr.A5850. Epub 2018 Nov 1. AJNR Am J Neuroradiol. 2018. PMID: 30385476 Free PMC article. No abstract available.
-
Application of 3D T1 Black-Blood Imaging in the Diagnosis of Leptomeningeal Carcinomatosis: Potential Pitfall of Slow-Flowing Blood.AJNR Am J Neuroradiol. 2018 Dec;39(12):E125. doi: 10.3174/ajnr.A5832. Epub 2018 Nov 1. AJNR Am J Neuroradiol. 2018. PMID: 30385477 Free PMC article. No abstract available.
References
-
- Chamberlain MC. Neoplastic meningitis. Neurologist 2006;12:179–87 10.1097/01.nrl.0000219732.33321.cc - DOI - PubMed
-
- Nakagawa H, Murasawa A, Kubo S, et al. Diagnosis and treatment of patients with meningeal carcinomatosis. J Neurooncol 1992;13:81–89 - PubMed
-
- Shapiro WR, Johanson CE, Boogerd W. Treatment modalities for leptomeningeal metastases. Semin Oncol 2008;36:S46–54 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical