

A Type 1 Diabetes Genetic Risk Score Predicts Progression of Islet Autoimmunity and Development of Type 1 Diabetes in Individuals at Risk
- PMID: 30002199
- PMCID: PMC6105323
- DOI: 10.2337/dc18-0087
A Type 1 Diabetes Genetic Risk Score Predicts Progression of Islet Autoimmunity and Development of Type 1 Diabetes in Individuals at Risk
Abstract
Objective: We tested the ability of a type 1 diabetes (T1D) genetic risk score (GRS) to predict progression of islet autoimmunity and T1D in at-risk individuals.
Research design and methods: We studied the 1,244 TrialNet Pathway to Prevention study participants (T1D patients' relatives without diabetes and with one or more positive autoantibodies) who were genotyped with Illumina ImmunoChip (median [range] age at initial autoantibody determination 11.1 years [1.2-51.8], 48% male, 80.5% non-Hispanic white, median follow-up 5.4 years). Of 291 participants with a single positive autoantibody at screening, 157 converted to multiple autoantibody positivity and 55 developed diabetes. Of 953 participants with multiple positive autoantibodies at screening, 419 developed diabetes. We calculated the T1D GRS from 30 T1D-associated single nucleotide polymorphisms. We used multivariable Cox regression models, time-dependent receiver operating characteristic curves, and area under the curve (AUC) measures to evaluate prognostic utility of T1D GRS, age, sex, Diabetes Prevention Trial-Type 1 (DPT-1) Risk Score, positive autoantibody number or type, HLA DR3/DR4-DQ8 status, and race/ethnicity. We used recursive partitioning analyses to identify cut points in continuous variables.
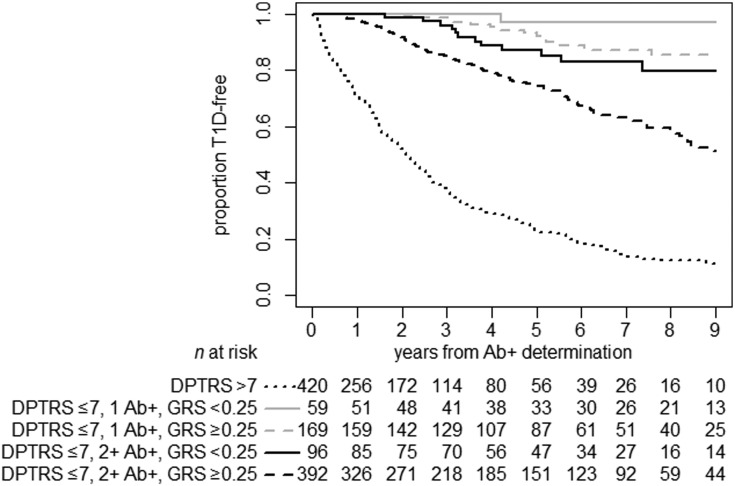
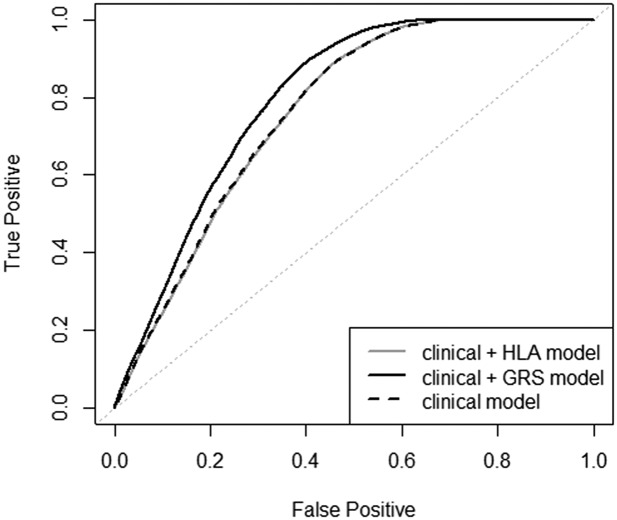
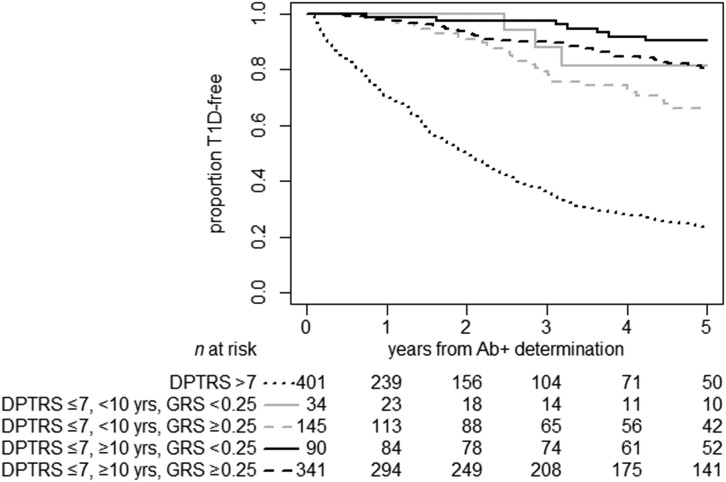
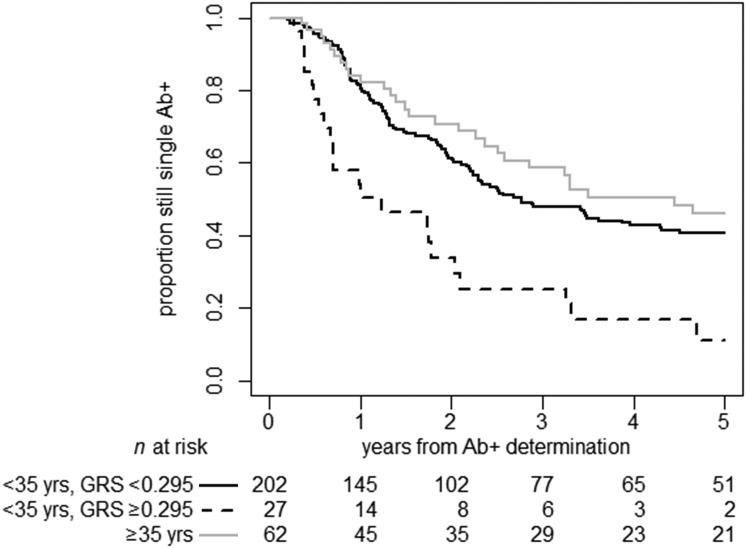
Results: Higher T1D GRS significantly increased the rate of progression to T1D adjusting for DPT-1 Risk Score, age, number of positive autoantibodies, sex, and ethnicity (hazard ratio [HR] 1.29 for a 0.05 increase, 95% CI 1.06-1.6; P = 0.011). Progression to T1D was best predicted by a combined model with GRS, number of positive autoantibodies, DPT-1 Risk Score, and age (7-year time-integrated AUC = 0.79, 5-year AUC = 0.73). Higher GRS was significantly associated with increased progression rate from single to multiple positive autoantibodies after adjusting for age, autoantibody type, ethnicity, and sex (HR 2.27 for GRS >0.295, 95% CI 1.47-3.51; P = 0.0002).
Conclusions: The T1D GRS independently predicts progression to T1D and improves prediction along T1D stages in autoantibody-positive relatives.
© 2018 by the American Diabetes Association.
Figures
References
-
- Mrena S, Virtanen SM, Laippala P, et al. Models for predicting type 1 diabetes in siblings of affected children. Diabetes Care 2006;29:662–667 - PubMed
-
- Sosenko JM, Krischer JP, Palmer JP, et al.; Diabetes Prevention Trial–Type 1 Study Group . A risk score for type 1 diabetes derived from autoantibody-positive participants in the Diabetes Prevention Trial–Type 1. Diabetes Care 2008;31:528–533 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 DK085476/DK/NIDDK NIH HHS/United States
- U01 DK061010/DK/NIDDK NIH HHS/United States
- P01 AI042288/AI/NIAID NIH HHS/United States
- U01 DK085453/DK/NIDDK NIH HHS/United States
- MC_PC_15047/MRC_/Medical Research Council/United Kingdom
- T32 DK065522/DK/NIDDK NIH HHS/United States
- U01 DK103282/DK/NIDDK NIH HHS/United States
- UC4 DK106993/DK/NIDDK NIH HHS/United States
- U01 DK061042/DK/NIDDK NIH HHS/United States
- U01 DK085509/DK/NIDDK NIH HHS/United States
- UC4 DK117009/DK/NIDDK NIH HHS/United States
- P30 DK017047/DK/NIDDK NIH HHS/United States
- U01 DK085466/DK/NIDDK NIH HHS/United States
- U01 DK103153/DK/NIDDK NIH HHS/United States
- U01 DK061058/DK/NIDDK NIH HHS/United States
- U01 DK106984/DK/NIDDK NIH HHS/United States
- U01 DK085499/DK/NIDDK NIH HHS/United States
- U01 DK107013/DK/NIDDK NIH HHS/United States
- U01 DK103266/DK/NIDDK NIH HHS/United States
- U01 DK107014/DK/NIDDK NIH HHS/United States
- U01 DK106994/DK/NIDDK NIH HHS/United States
- U01 DK061034/DK/NIDDK NIH HHS/United States
- U01 DK085461/DK/NIDDK NIH HHS/United States
- U01 DK103180/DK/NIDDK NIH HHS/United States
- U01 DK085465/DK/NIDDK NIH HHS/United States
- U01 DK085504/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
