

Uterine artery pseudoaneurysm with an anastomotic feeding vessel requiring repeat embolisation
- PMID: 30002208
- PMCID: PMC6047716
- DOI: 10.1136/bcr-2018-224656
Uterine artery pseudoaneurysm with an anastomotic feeding vessel requiring repeat embolisation
Abstract
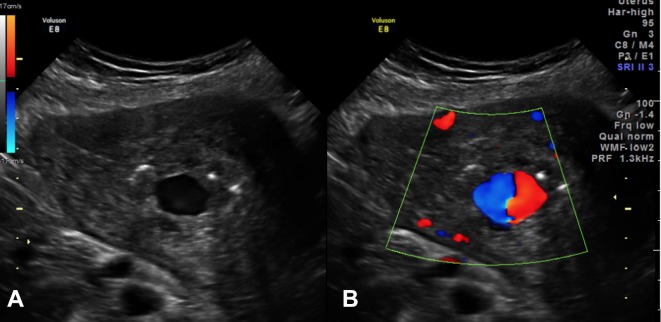
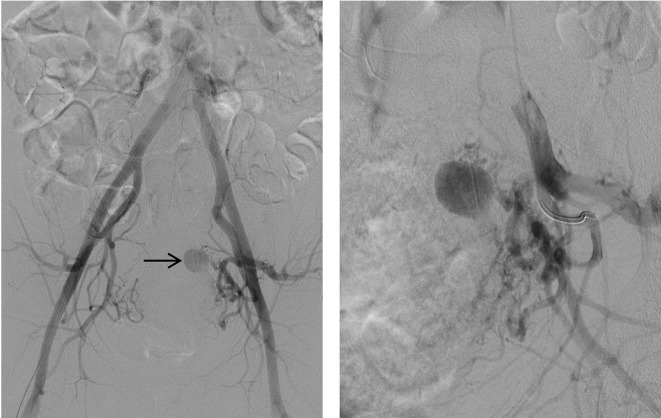
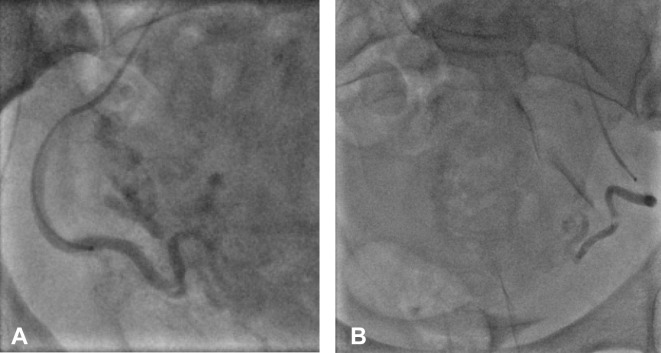
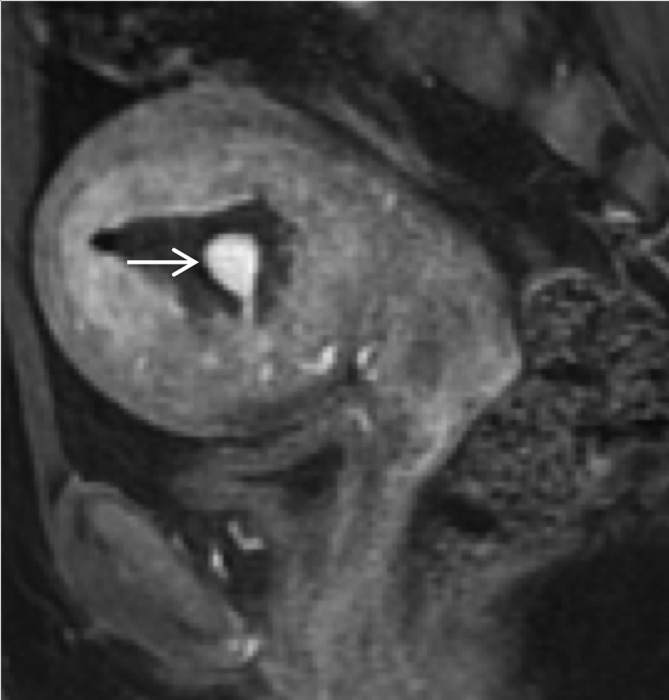
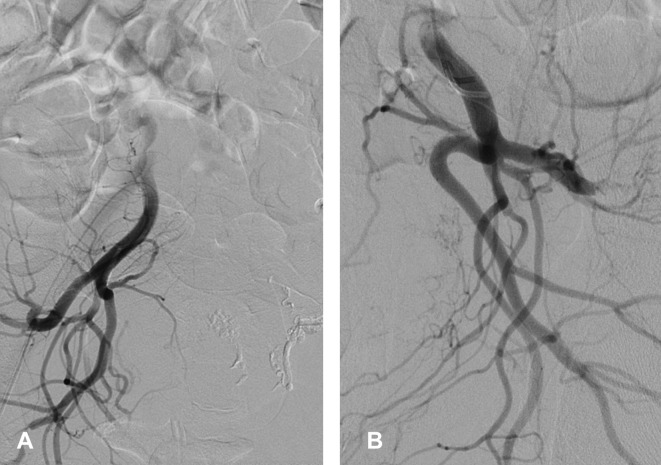
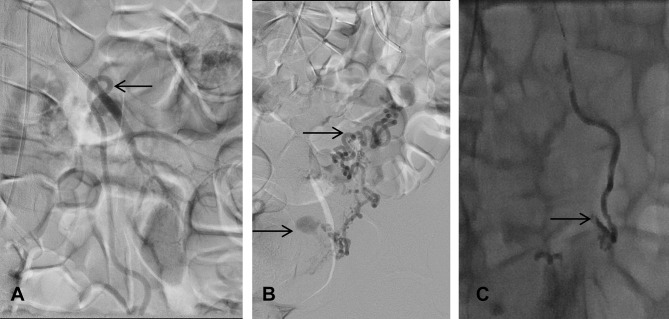
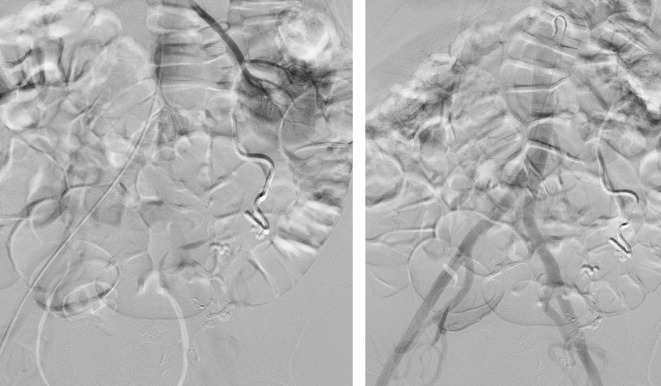
Uterine artery pseudoaneurysm (UAP) is a rare cause of delayed postpartum haemorrhage. Early diagnosis and endovascular management are effective in treating this condition. We present the case of a 36-year-old gravida 3, para 2 woman with delayed postpartum haemorrhage and endometritis following a spontaneous vaginal delivery. Ultrasound and catheter angiogram demonstrated a UAP arising from the distal aspect of the left uterine artery. Significant bleed persisted despite selective bilateral uterine artery embolisation. A repeat angiogram confirmed complete occlusion of bilateral uterine arteries, but abdominal aortogram demonstrated that the left ovarian artery was now feeding the pseudoaneurysm. A repeat embolisation procedure was performed to occlude the left ovarian artery. The patient was discharged the following day. Selective arterial embolisation is effective in the management of UAP. Persistent bleeding despite embolisation should raise the suspicion of anastomotic vascular supply and may require repeat embolisation.
Keywords: interventional radiology; obstetrics, gynaecology and fertility; pregnancy.
© BMJ Publishing Group Limited 2018. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Case of postpartum uterine artery pseudoaneurysm associated with von Willebrand disease.BMJ Case Rep. 2022 Dec 23;15(12):e253804. doi: 10.1136/bcr-2022-253804. BMJ Case Rep. 2022. PMID: 36564091 Free PMC article.
-
Pseudoaneurysm of uterine artery complicating caesarean section: a rare cause of intractable secondary postpartum haemorrhage managed with uterine artery embolisation.BMJ Case Rep. 2021 Mar 22;14(3):e239851. doi: 10.1136/bcr-2020-239851. BMJ Case Rep. 2021. PMID: 33753382 Free PMC article.
-
Modified sandwich embolization technique for postpartum hemorrhage caused by uterine artery pseudoaneurysm: a case series.Arch Gynecol Obstet. 2020 Dec;302(6):1469-1477. doi: 10.1007/s00404-020-05786-x. Epub 2020 Sep 10. Arch Gynecol Obstet. 2020. PMID: 32914223
-
Severe Postcoital Bleeding From a Uterine Artery Pseudoaneurysm 4 Months After Cesarean Delivery.Obstet Gynecol. 2015 Sep;126(3):638-641. doi: 10.1097/AOG.0000000000000849. Obstet Gynecol. 2015. PMID: 26132452 Review.
-
Extravasating uterine pseudoaneurysm: A rare cause of postpartum haemorrhage.J Obstet Gynaecol. 2017 May;37(4):416-420. doi: 10.1080/01443615.2016.1274292. Epub 2017 Feb 25. J Obstet Gynaecol. 2017. PMID: 28421908 Review.
Cited by
-
Spontaneous Rupture of a Right Gonadal Artery Aneurysm: A Case Report.Cureus. 2024 Mar 31;16(3):e57352. doi: 10.7759/cureus.57352. eCollection 2024 Mar. Cureus. 2024. PMID: 38694409 Free PMC article.
-
Recurrent uterine artery pseudo-aneurysm requiring repeat embolization during pregnancy - A case report.Case Rep Womens Health. 2020 Dec 14;29:e00280. doi: 10.1016/j.crwh.2020.e00280. eCollection 2021 Jan. Case Rep Womens Health. 2020. PMID: 33457211 Free PMC article.
-
Uterine Artery Pseudoaneurysm after an Uncomplicated Vaginal Delivery: A Case Report.Clin Pract. 2022 Oct 12;12(5):826-831. doi: 10.3390/clinpract12050087. Clin Pract. 2022. PMID: 36286073 Free PMC article.
References
-
- Combs CA, Murphy EL, Laros RK. Factors associated with postpartum hemorrhage with vaginal birth. Obstet Gynecol 1991;77:69–76. - PubMed
-
- Khong TY, Khong TK. Delayed postpartum hemorrhage: a morphologic study of causes and their relation to other pregnancy disorders. Obstet Gynecol 1993;82:17–22. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical