

Assessment of Lung Cancer Risk on the Basis of a Biomarker Panel of Circulating Proteins
- PMID: 30003238
- PMCID: PMC6233784
- DOI: 10.1001/jamaoncol.2018.2078
Assessment of Lung Cancer Risk on the Basis of a Biomarker Panel of Circulating Proteins
Erratum in
-
Incorrect Author Surname.JAMA Oncol. 2018 Oct 1;4(10):1439. doi: 10.1001/jamaoncol.2018.4576. JAMA Oncol. 2018. PMID: 30242395 Free PMC article. No abstract available.
-
Failure to Disclose a Potential Conflict of Interest.JAMA Oncol. 2019 Dec 1;5(12):1811. doi: 10.1001/jamaoncol.2019.5468. JAMA Oncol. 2019. PMID: 31725820 Free PMC article. No abstract available.
Abstract
Importance: There is an urgent need to improve lung cancer risk assessment because current screening criteria miss a large proportion of cases.
Objective: To investigate whether a lung cancer risk prediction model based on a panel of selected circulating protein biomarkers can outperform a traditional risk prediction model and current US screening criteria.
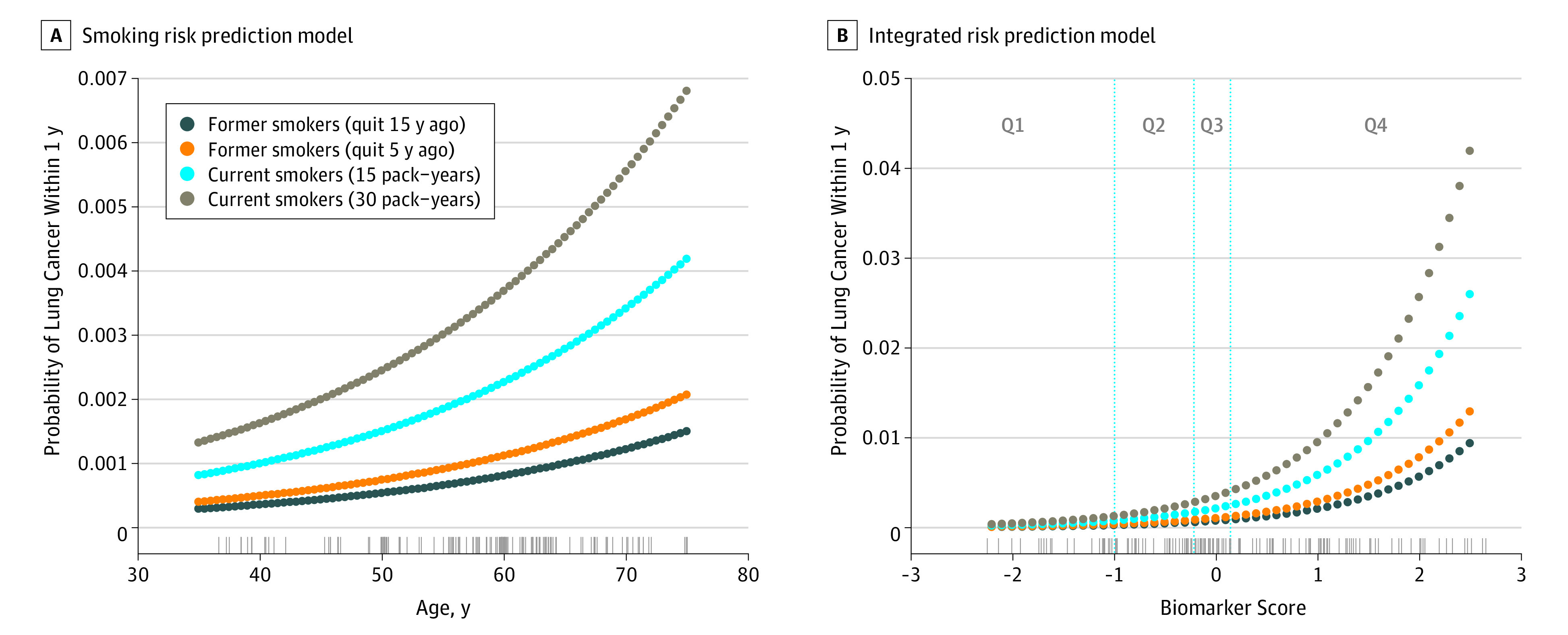
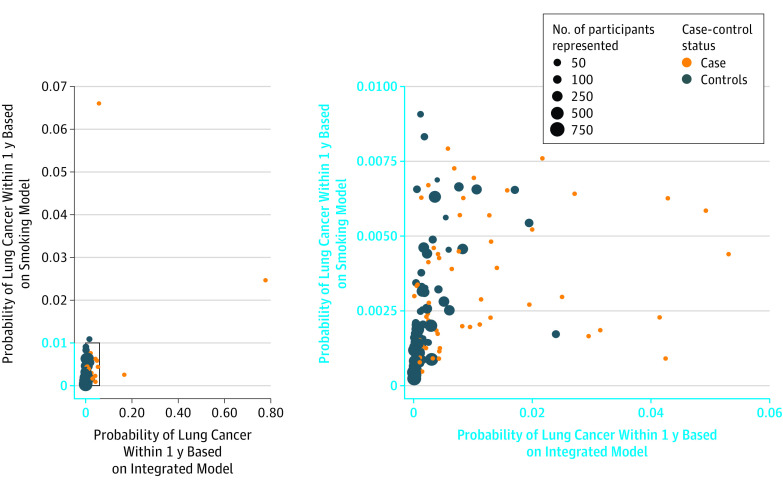
Design, setting, and participants: Prediagnostic samples from 108 ever-smoking patients with lung cancer diagnosed within 1 year after blood collection and samples from 216 smoking-matched controls from the Carotene and Retinol Efficacy Trial (CARET) cohort were used to develop a biomarker risk score based on 4 proteins (cancer antigen 125 [CA125], carcinoembryonic antigen [CEA], cytokeratin-19 fragment [CYFRA 21-1], and the precursor form of surfactant protein B [Pro-SFTPB]). The biomarker score was subsequently validated blindly using absolute risk estimates among 63 ever-smoking patients with lung cancer diagnosed within 1 year after blood collection and 90 matched controls from 2 large European population-based cohorts, the European Prospective Investigation into Cancer and Nutrition (EPIC) and the Northern Sweden Health and Disease Study (NSHDS).
Main outcomes and measures: Model validity in discriminating between future lung cancer cases and controls. Discrimination estimates were weighted to reflect the background populations of EPIC and NSHDS validation studies (area under the receiver-operating characteristics curve [AUC], sensitivity, and specificity).
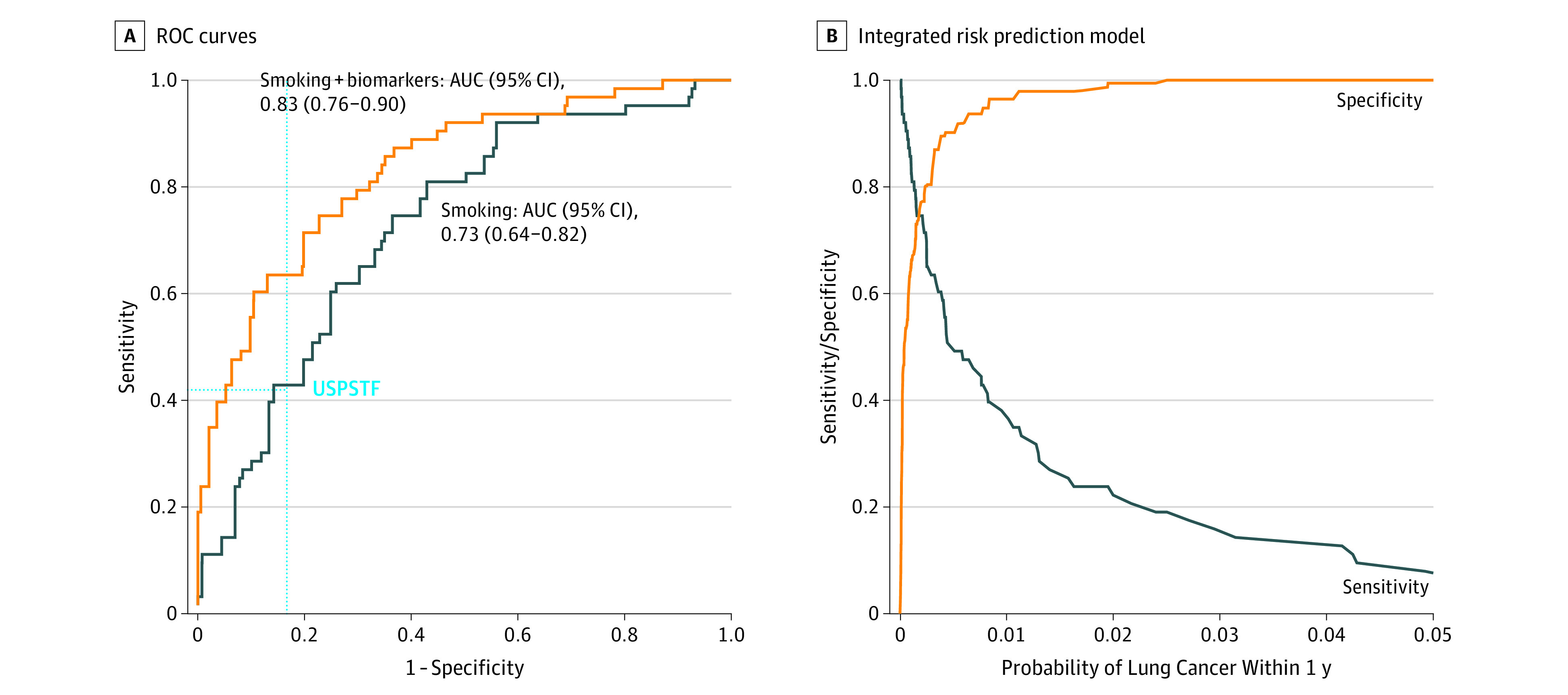
Results: In the validation study of 63 ever-smoking patients with lung cancer and 90 matched controls (mean [SD] age, 57.7 [8.7] years; 68.6% men) from EPIC and NSHDS, an integrated risk prediction model that combined smoking exposure with the biomarker score yielded an AUC of 0.83 (95% CI, 0.76-0.90) compared with 0.73 (95% CI, 0.64-0.82) for a model based on smoking exposure alone (P = .003 for difference in AUC). At an overall specificity of 0.83, based on the US Preventive Services Task Force screening criteria, the sensitivity of the integrated risk prediction (biomarker) model was 0.63 compared with 0.43 for the smoking model. Conversely, at an overall sensitivity of 0.42, based on the US Preventive Services Task Force screening criteria, the integrated risk prediction model yielded a specificity of 0.95 compared with 0.86 for the smoking model.
Conclusions and relevance: This study provided a proof of principle in showing that a panel of circulating protein biomarkers may improve lung cancer risk assessment and may be used to define eligibility for computed tomography screening.
Conflict of interest statement
Figures
Comment in
-
A novel biomarker protein panel for lung cancer, a promising first step.Transl Lung Cancer Res. 2018 Dec;7(Suppl 4):S304-S307. doi: 10.21037/tlcr.2018.12.09. Transl Lung Cancer Res. 2018. PMID: 30705841 Free PMC article. No abstract available.
-
Failure to Disclose Potential Conflict of Interest-Letter of Explanation.JAMA Oncol. 2019 Dec 1;5(12):1811. doi: 10.1001/jamaoncol.2019.5259. JAMA Oncol. 2019. PMID: 31725855 No abstract available.
References
-
- Humphrey L, Deffebach M, Pappas M, et al. Screening for Lung Cancer. Rockville, MD: Systematic Review to Update the US Preventive Services Task Force Recommendation; 2013. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
- Andalusian Health Repository - access to free full text
- Archivio Istituzionale della Ricerca Unimi - Access Free Full Text
- Diposit Digital de la Universitat de Barcelona - Access Free Full Text
- Europe PubMed Central
- Ovid Technologies, Inc.
- PubMed Central
- Silverchair Information Systems
- Spiral, Imperial College Digital Repository
Other Literature Sources
Medical
Research Materials
Miscellaneous
