

Budd-Chiari syndrome: imaging review
- PMID: 30004805
- PMCID: PMC6319835
- DOI: 10.1259/bjr.20180441
Budd-Chiari syndrome: imaging review
Abstract
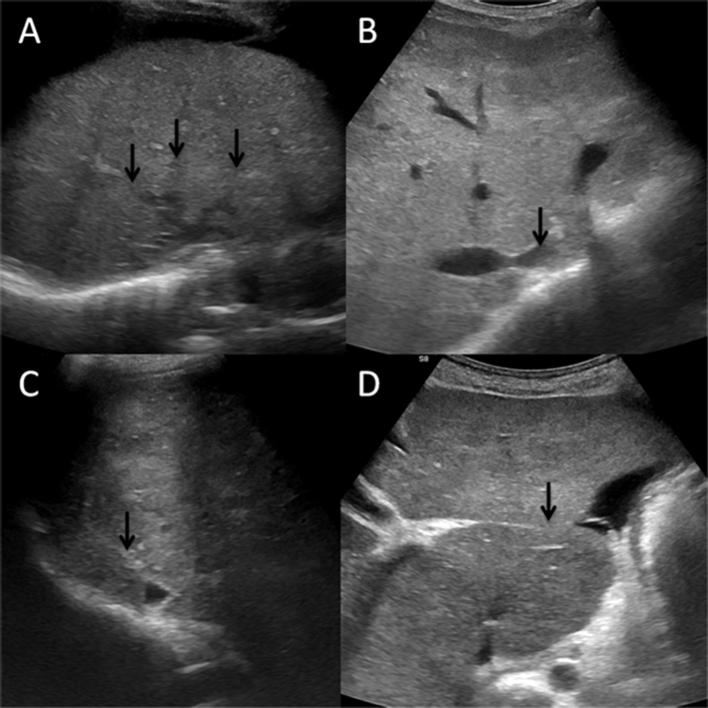
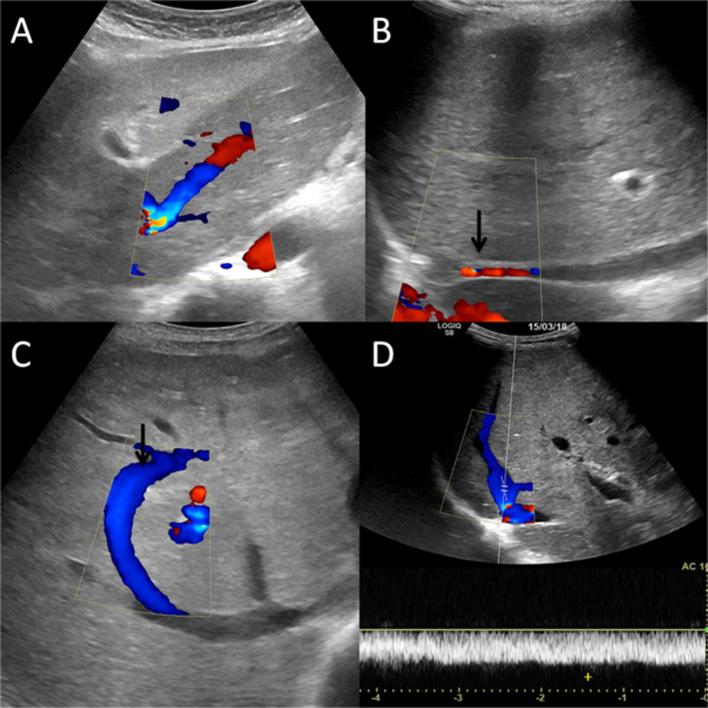
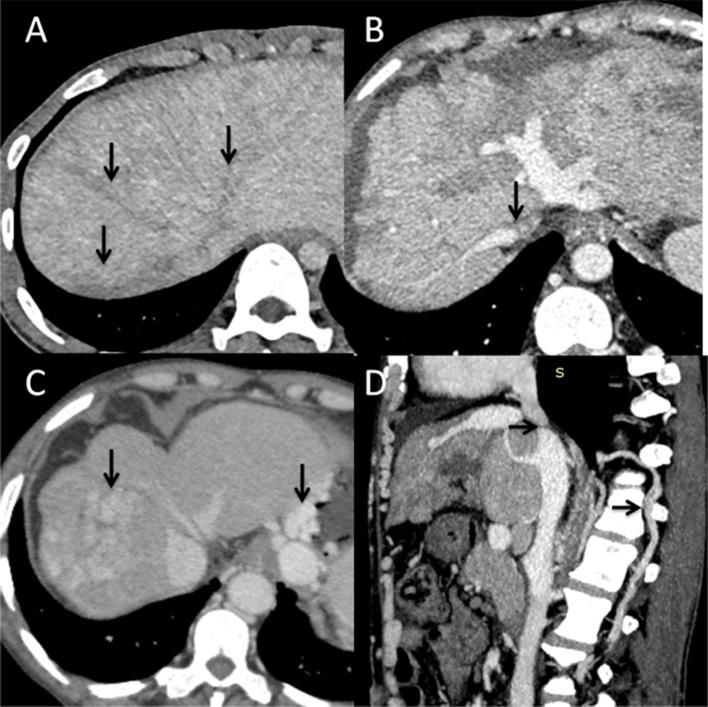
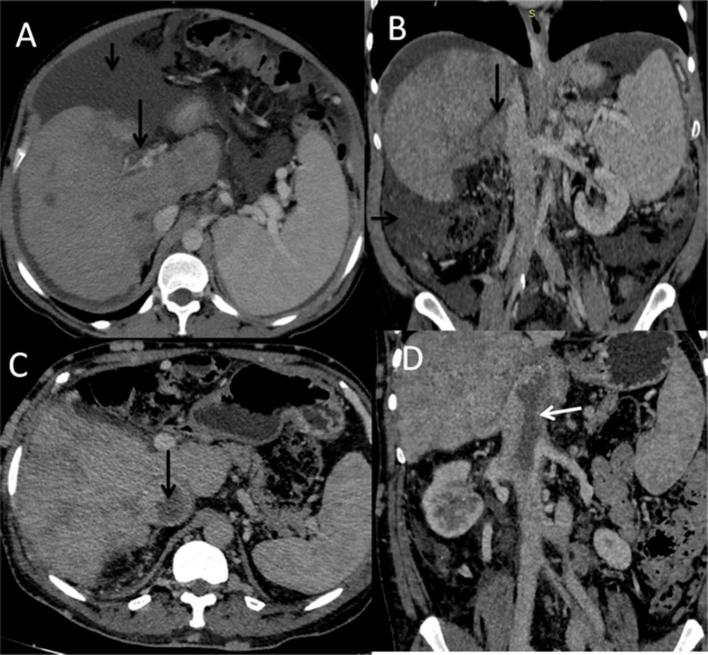
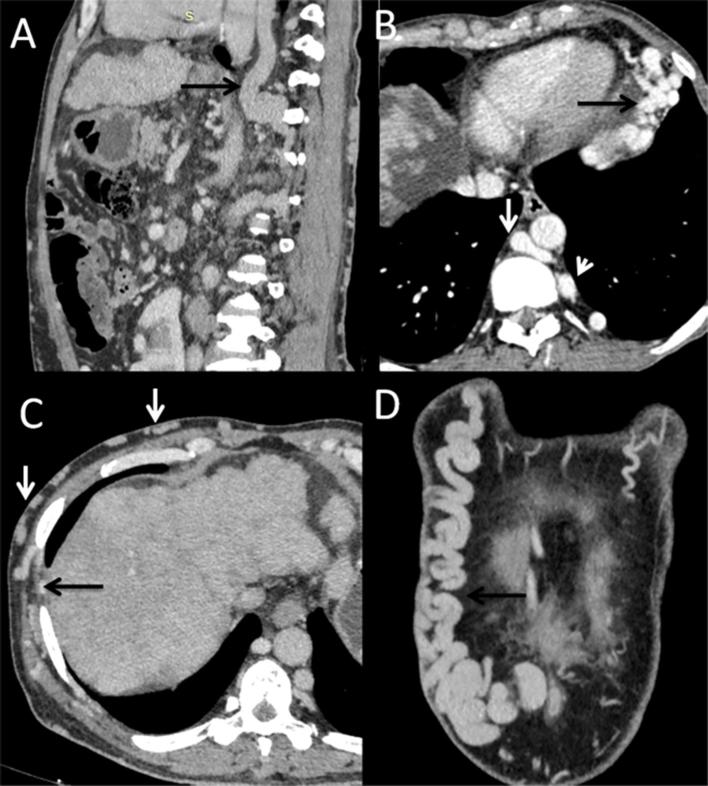
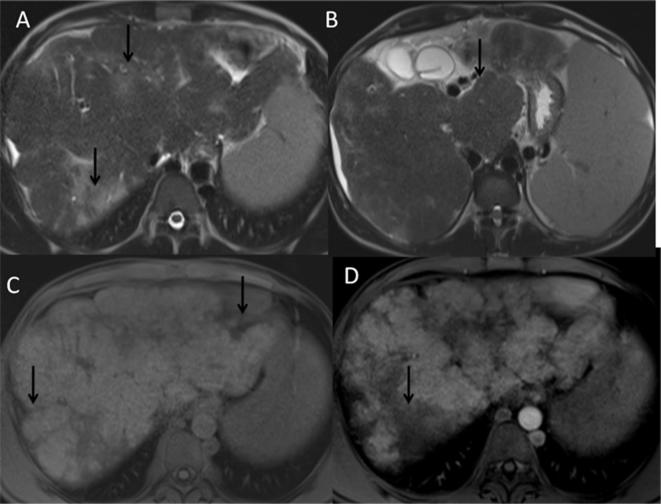
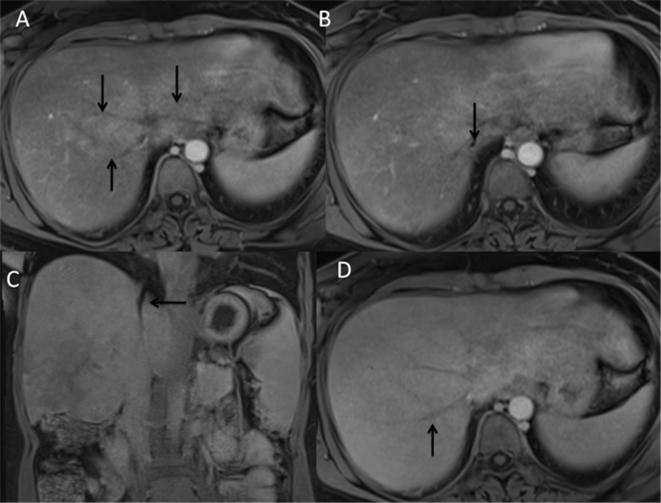
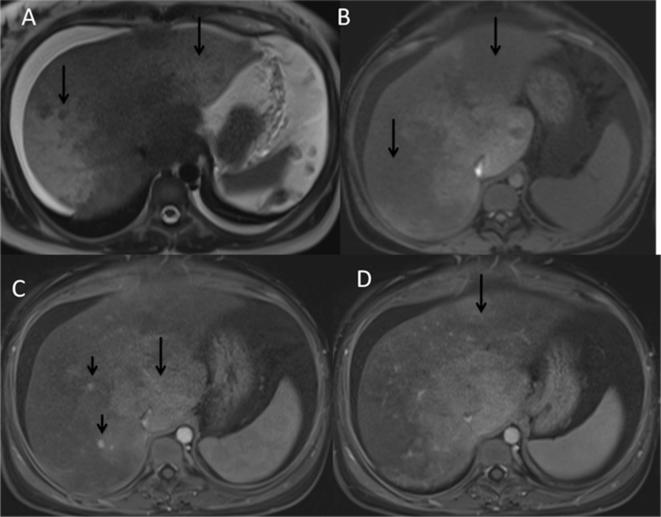
Budd-Chiari syndrome (BCS), also known as hepatic venous outflow tract obstruction includes a group of conditions characterized by obstruction to the outflow of blood from the liver secondary to involvement of one or more hepatic veins (HVs), inferior vena cava (IVC) or the right atrium. There are a number of conditions that lead to BCS-ranging from hypercoagulable states to malignancies. In up to 25% patients, no underlying disorder is identified. Diagnosis of BCS is based on a combination of clinical and imaging features. A major part of the literature in BCS has been devoted to interventions; however, a detailed description of various imaging manifestations of BCS is lacking. In this review, we highlight the importance of various imaging modalities in the diagnosis of BCS.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
