

Noninvasive wave intensity analysis predicts functional worsening in children with pulmonary arterial hypertension
- PMID: 30004811
- PMCID: PMC6737454
- DOI: 10.1152/ajpheart.00227.2018
Noninvasive wave intensity analysis predicts functional worsening in children with pulmonary arterial hypertension
Abstract
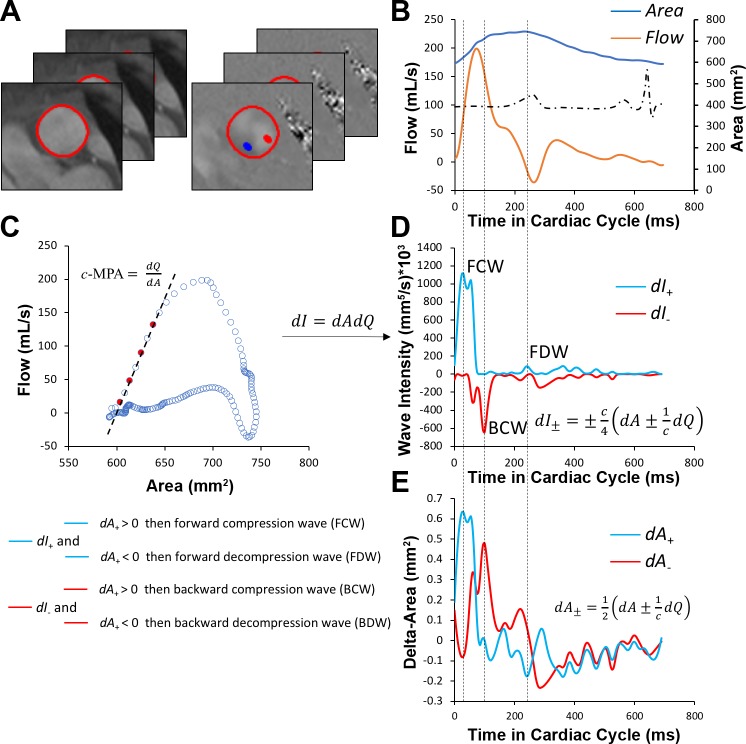
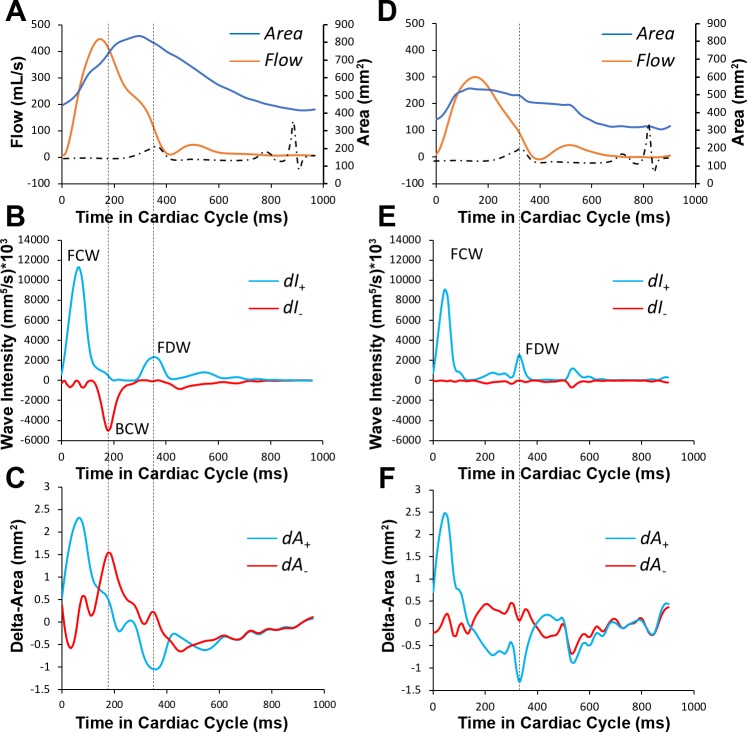
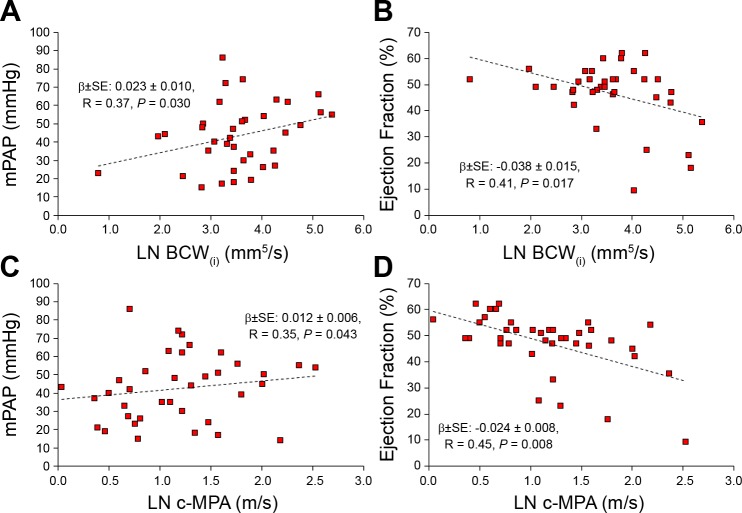
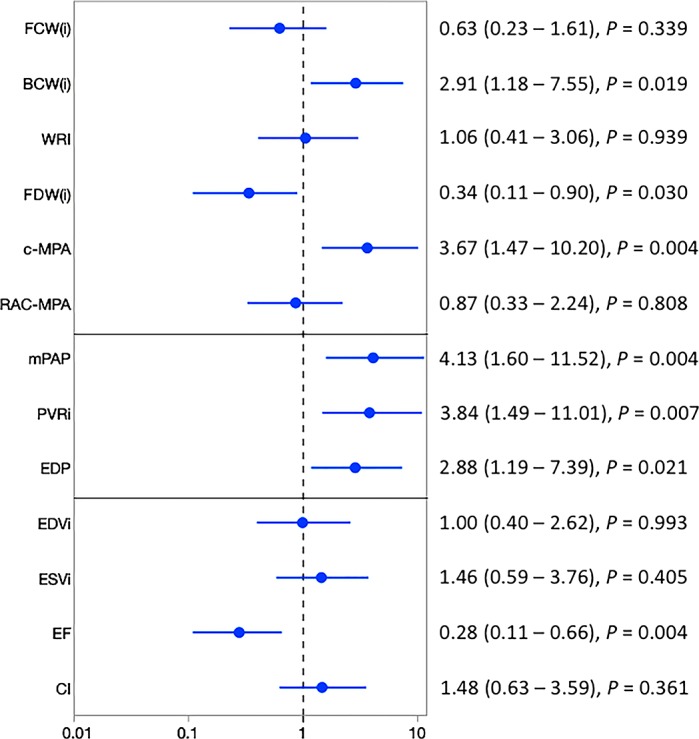
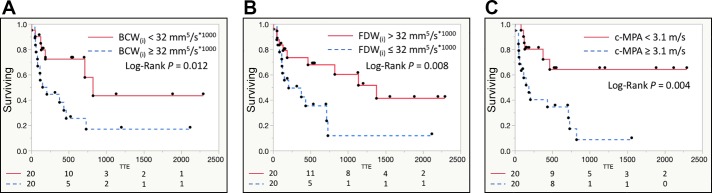
The purpose of the present study was to characterize pulmonary vascular stiffness using wave intensity analysis (WIA) in children with pulmonary arterial hypertension (PAH), compare the WIA indexes with catheterization- and MRI-derived hemodynamics, and assess the prognostic ability of WIA-derived biomarkers to predict the functional worsening. WIA was performed in children with PAH ( n = 40) and healthy control subjects ( n = 15) from phase-contrast MRI-derived flow and area waveforms in the main pulmonary artery (MPA). From comprehensive WIA spectra, we collected and compared with healthy control subjects forward compression waves (FCW), backward compression waves (BCW), forward decompression waves (FDW), and wave propagation speed ( c-MPA). There was no difference in the magnitude of FCW between PAH and control groups (88 vs. 108 mm5·s-1·ml-1, P = 0.239). The magnitude of BCW was increased in patients with PAH (32 vs. 5 mm5·s-1·ml-1, P < 0.001). There was no difference in magnitude of indexed FDW (32 vs. 28 mm5·s-1·ml-1, P = 0.856). c-MPA was increased in patients with PAH (3.2 vs. 1.6 m/s, P < 0.001). BCW and FCW correlated with mean pulmonary arterial pressure, right ventricular volumes, and ejection fraction. Elevated indexed BCW [heart rate (HR) = 2.91, confidence interval (CI): 1.18-7.55, P = 0.019], reduced indexed FDW (HR = 0.34, CI: 0.11-0.90, P = 0.030), and increased c-MPA (HR = 3.67, CI: 1.47-10.20, P = 0.004) were strongly associated with functional worsening of disease severity. Our results suggest that noninvasively derived biomarkers of pulmonary vascular resistance and stiffness may be helpful for determining prognosis and monitoring disease progression in children with PAH. NEW & NOTEWORTHY Wave intensity analysis (WIA) studies are lacking in children with pulmonary arterial hypertension (PAH) partially because WIA, which is necessary to assess vascular stiffness, requires an invasive pressure-derived waveform along with simultaneous flow measurements. We analyzed vascular stiffness using WIA in children with PAH who underwent phase-contrast MRI and observed significant differences in WIA indexes between patients with PAH and control subjects. Furthermore, WIA indexes were predictive of functional worsening and were associated with standard catheterization measures.
Keywords: magnetic resonance imaging; pediatric pulmonary arterial hypertension; vascular stiffness.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- Abman SH, Hansmann G, Archer SL, Ivy DD, Adatia I, Chung WK, Hanna BD, Rosenzweig EB, Raj JU, Cornfield D, Stenmark KR, Steinhorn R, Thébaud B, Fineman JR, Kuehne T, Feinstein JA, Friedberg MK, Earing M, Barst RJ, Keller RL, Kinsella JP, Mullen M, Deterding R, Kulik T, Mallory G, Humpl T, Wessel DL; American Heart Association Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation; Council on Clinical Cardiology; Council on Cardiovascular Disease in the Young; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Surgery and Anesthesia; American Thoracic Society . Pediatric pulmonary hypertension: guidelines from the American Heart Association and American Thoracic Society. Circulation 132: 2037–2099, 2015. [Erratum in Circulation 133: e368, 2016. doi: 10.1161/CIR.0000000000000363.] doi: 10.1161/CIR.0000000000000329. - DOI - PubMed
-
- Biglino G, Schievano S, Steeden JA, Ntsinjana H, Baker C, Khambadkone S, de Leval MR, Hsia TY, Taylor AM, Giardini A; Modeling of Congenital Hearts Alliance (MOCHA) Collaborative Group . Reduced ascending aorta distensibility relates to adverse ventricular mechanics in patients with hypoplastic left heart syndrome: noninvasive study using wave intensity analysis. J Thorac Cardiovasc Surg 144: 1307–1314, 2012. doi: 10.1016/j.jtcvs.2012.08.028. - DOI - PubMed
-
- Burkett DA, Slorach C, Patel SS, Redington AN, Ivy DD, Mertens L, Younoszai AK, Friedberg MK. Impact of pulmonary hemodynamics and ventricular interdependence on left ventricular diastolic function in children with pulmonary hypertension. Circ Cardiovasc Imaging 9: e004612, 2016. doi: 10.1161/CIRCIMAGING.116.004612. - DOI - PMC - PubMed
-
- Davies JE, Alastruey J, Francis DP, Hadjiloizou N, Whinnett ZI, Manisty CH, Aguado-Sierra J, Willson K, Foale RA, Malik IS, Hughes AD, Parker KH, Mayet J. Attenuation of wave reflection by wave entrapment creates a “horizon effect” in the human aorta. Hypertension 60: 778–785, 2012. doi: 10.1161/HYPERTENSIONAHA.111.180604. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical