

Prognostic value of platelet count and lymphocyte to monocyte ratio combination in stage IV non-small cell lung cancer with malignant pleural effusion
- PMID: 30005083
- PMCID: PMC6044534
- DOI: 10.1371/journal.pone.0200341
Prognostic value of platelet count and lymphocyte to monocyte ratio combination in stage IV non-small cell lung cancer with malignant pleural effusion
Abstract
Introduction: A combination of platelet and lymphocyte to monocyte ratio (LMR) (abbreviated as COP-LMR) has been recently evaluated as systemic inflammatory marker for prognostication in lung cancer. While previous study on COP-LMR has evaluated its prognostic value in NSCLC patients who underwent curative resections, the combination of these two markers has not been evaluated in advanced NSCLC yet.
Objectives: In this study, we evaluated the prognostic value of COP-LMR in stage IV NSCLC with malignant pleural effusion under active anticancer treatment.
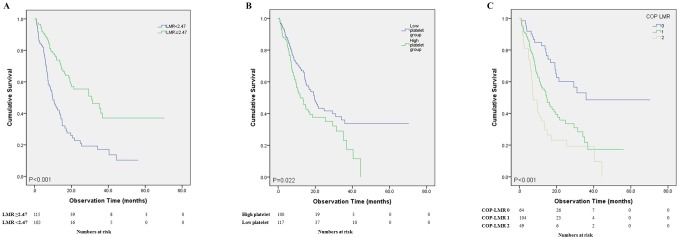
Methods: Between January 2012 and July 2016, 217 patients with stage IV NSCLC and MPE undergoing active anticancer treatment were selected for evaluation. If patients had both low LMR (< 2.47) and increased platelet (> 30.0 ×10(4) mm-3), they were assigned to COP-LMR group 2. Patients with one parameter were assigned to COP-LMR group 1. If none, patients were assigned to COP-LMR group 0.
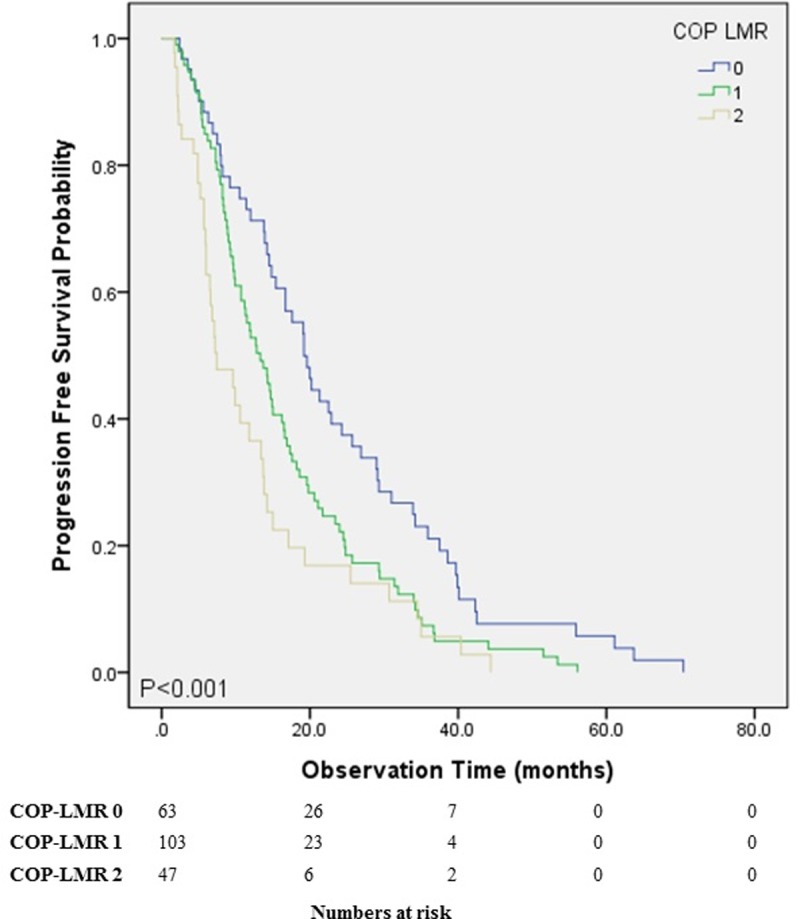
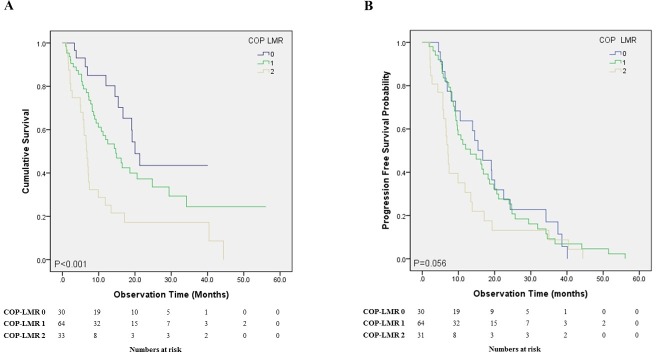
Results: Median overall survival (OS) (P < 0.001), progression free survival (PFS) (P < 0.001) and histological feature (P = 0.003) showed significant differences among COP-LMR groups. For COP-LMR groups 0, 1 and 2, median survival times were 35.9, 14.7 and 7.4 months, respectively, while median progression free times were 19.2, 13.3 and 7.4 months, respectively. Older age, male, low albumin, high CRP and high COP-LMR (0 vs 1, P = 0.021, hazard ratio (HR): 1.822, 95% confidence interval (CI): 1.096-3.027 and 0 vs 2, P = 0.003, HR: 2.464, 95% CI: 1.373-4.421) were independent predictive factors for shorter OS. Age, sex, histology, albumin, or CRP had no significant influence on PFS. High COP-LMR was the significant factor in predicting shorter PFS (0 vs 1, P = 0.116 and 0 vs 2, P = 0.007, HR: 1.902, 95% CI: 1.194-3.028).
Conclusions: A combination of pretreatment LMR and platelet levels can be used to predict short survival in stage IV NSCLC patients who underwent active anticancer treatment.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Moro-Sibilot D, Smit E, de Castro Carpeno J, Lesniewski-Kmak K, Aerts J, Villatoro R, et al. Outcomes and resource use of non-small cell lung cancer (NSCLC) patients treated with first-line platinum-based chemotherapy across Europe: FRAME prospective observational study. Lung Cancer. 2015;88(2):215–22. 10.1016/j.lungcan.2015.02.011 . - DOI - PubMed
-
- O'Callaghan DS, O'Donnell D, O'Connell F, O'Byrne KJ. The role of inflammation in the pathogenesis of non-small cell lung cancer. J Thorac Oncol. 2010;5(12):2024–36. . - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
