

Sex and Race Differences in the Utilization and Outcomes of Coronary Artery Bypass Grafting Among Medicare Beneficiaries, 1999-2014
- PMID: 30005557
- PMCID: PMC6064835
- DOI: 10.1161/JAHA.118.009014
Sex and Race Differences in the Utilization and Outcomes of Coronary Artery Bypass Grafting Among Medicare Beneficiaries, 1999-2014
Abstract
Background: With over a decade of directed efforts to reduce sex and racial differences in coronary artery bypass grafting (CABG) utilization, and post-CABG outcomes, we sought to evaluate how the use of CABG and its outcomes have evolved in different sex and racial subgroups.
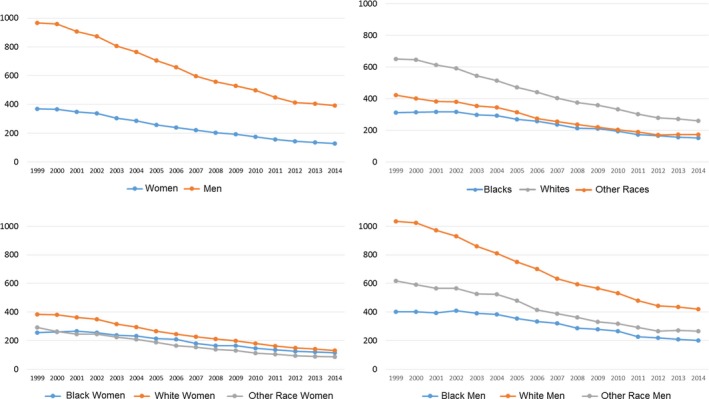
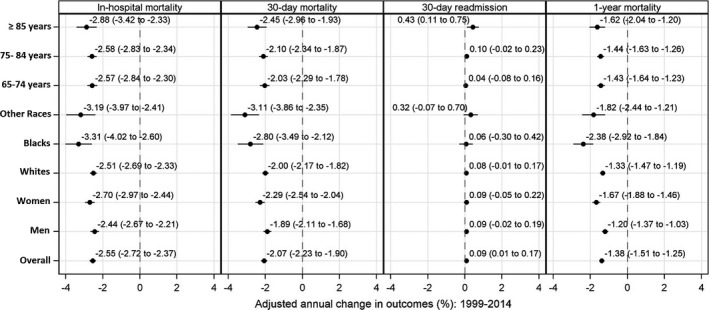
Methods and results: Using data on all fee-for-service Medicare beneficiaries undergoing CABG in the United States from 1999 to 2014, we examined differences by sex and race in calendar-year trends for CABG utilization and post-CABG outcomes (in-hospital, 30-day, and 1-year mortality and 30-day readmission). A total of 1 863 719 Medicare fee-for-service beneficiaries (33.6% women, 4.6% black) underwent CABG from 1999 to 2014, with a decrease from 611 to 245 CABG procedures per 100 000 person-years. Men compared with women and whites compared with blacks had higher CABG utilization, with declines in all subgroups. Higher post-CABG annual declines in mortality (95% confidence interval) were observed in women (in-hospital, -2.70% [-2.97, -2.44]; 30-day, -2.29% [-2.54, -2.04]; and 1-year mortality, -1.67% [-1.88, -1.46]) and blacks (in-hospital, -3.31% [-4.02, -2.60]; 30-day, -2.80% [-3.49, -2.12]; and 1-year mortality, -2.38% [-2.92, -1.84]), compared with men and whites, respectively. Mortality rates remained higher in women and blacks, but differences narrowed over time. Annual adjusted 30-day readmission rates remained unchanged for all patient groups.
Conclusions: Women and black patients had persistently higher CABG mortality than men and white patients, respectively, despite greater declines over the time period. These findings indicate progress, but also the need for further progress.
Keywords: bypass graft; mortality; race; readmission; sex.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Similar articles
-
Trends in In-hospital Coronary Artery Bypass Surgery Mortality by Gender and Race/Ethnicity --1998-2015: Why Do the Differences Remain?J Natl Med Assoc. 2019 Oct;111(5):527-539. doi: 10.1016/j.jnma.2019.04.009. Epub 2019 Jun 4. J Natl Med Assoc. 2019. PMID: 31174847
-
Race, neighborhood disadvantage, and survival of Medicare beneficiaries after aortic valve replacement and concomitant coronary artery bypass grafting.J Thorac Cardiovasc Surg. 2024 Jun;167(6):2076-2090.e19. doi: 10.1016/j.jtcvs.2023.02.005. Epub 2023 Feb 13. J Thorac Cardiovasc Surg. 2024. PMID: 36894351
-
Racial disparity in the relationship between hospital volume and mortality among patients undergoing coronary artery bypass grafting.Ann Surg. 2008 Nov;248(5):886-92. doi: 10.1097/SLA.0b013e318189b1bc. Ann Surg. 2008. PMID: 18948819
-
Outcomes in Women Undergoing Coronary Artery Bypass Grafting: Analysis of New Data and Operative Trends.J Cardiothorac Vasc Anesth. 2025 Feb;39(2):532-537. doi: 10.1053/j.jvca.2024.10.031. Epub 2024 Oct 23. J Cardiothorac Vasc Anesth. 2025. PMID: 39547868 Review.
-
Sex differences in coronary artery bypass graft surgery outcomes: a narrative review.J Thorac Dis. 2023 Sep 28;15(9):5041-5054. doi: 10.21037/jtd-23-294. Epub 2023 Aug 16. J Thorac Dis. 2023. PMID: 37868858 Free PMC article. Review.
Cited by
-
Risk predictors of race disparity in patients undergoing coronary artery bypass grafting: a propensity-matched analysis.Interdiscip Cardiovasc Thorac Surg. 2024 Jan 2;38(1):ivae002. doi: 10.1093/icvts/ivae002. Interdiscip Cardiovasc Thorac Surg. 2024. PMID: 38180892 Free PMC article.
-
Persistent Racial and Sex Disparities in Outcomes After Coronary Artery Bypass Surgery: A Retrospective Clinical Registry Review in the Drug-eluting Stent Era.Ann Surg. 2020 Oct;272(4):660-667. doi: 10.1097/SLA.0000000000004335. Ann Surg. 2020. PMID: 32932322 Free PMC article.
-
Disparities in the Use of Cardiac Rehabilitation in African Americans.Curr Cardiovasc Risk Rep. 2022;16(5):31-41. doi: 10.1007/s12170-022-00690-2. Epub 2022 May 7. Curr Cardiovasc Risk Rep. 2022. PMID: 35573267 Free PMC article. Review.
-
Bias in Care: Impact of Ethnicity on Time to Emergent Surgery Varies Between Subspecialties.J Am Acad Orthop Surg Glob Res Rev. 2023 Jun 13;7(6):e23.00060. doi: 10.5435/JAAOSGlobal-D-23-00060. eCollection 2023 Jun 1. J Am Acad Orthop Surg Glob Res Rev. 2023. PMID: 37311114 Free PMC article.
-
Causal fairness assessment of treatment allocation with electronic health records.J Biomed Inform. 2024 Jul;155:104656. doi: 10.1016/j.jbi.2024.104656. Epub 2024 May 21. J Biomed Inform. 2024. PMID: 38782170 Free PMC article.
References
-
- Weiss A, Elixhauser A. Trends in operating room procedures in U.S. hospitals, 2001–2011: Statistical Brief #171. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs: Agency for Healthcare Research and Quality (US); 2014.
-
- Weiss A, Elixhauser A, Andrews R. Characteristics of operating room procedures in U.S. hospitals, 2011: Statistical Brief #170. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs: Agency for Healthcare Research and Quality (US); 2014. - PubMed
-
- Bridges CR, Edwards FH, Peterson ED, Coombs LP. The effect of race on coronary bypass operative mortality. J Am Coll Cardiol. 2000;36:1870–1876. - PubMed
-
- Castellanos LR, Li Z, Yeo KK, Young JN, Ayanian JZ, Amsterdam EA. Relation of race, ethnicity and cardiac surgeons to operative mortality rates in primary coronary artery bypass grafting in California. Am J Cardiol. 2011;107:1–5. - PubMed
-
- Hartz RS, Rao AV, Plomondon ME, Grover FL, Shroyer AL. Effects of race, with or without gender, on operative mortality after coronary artery bypass grafting: a study using the Society of Thoracic Surgeons national database. Ann Thorac Surg. 2001;71:512–520. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
