

A hospital-wide evaluation of delirium prevalence and outcomes in acute care patients - a cohort study
- PMID: 30005646
- PMCID: PMC6045819
- DOI: 10.1186/s12913-018-3345-x
A hospital-wide evaluation of delirium prevalence and outcomes in acute care patients - a cohort study
Abstract
Background: Delirium is a well-known complication in cardiac surgery and intensive care unit (ICU) patients. However, in many other settings its prevalence and clinical consequences are understudied. The aims of this study were: (1) To assess delirium prevalence in a large, diverse cohort of acute care patients classified as either at risk or not at risk for delirium; (2) To compare these two groups according to defined indicators; and (3) To compare delirious with non-delirious patients regarding hospital mortality, ICU and hospital length of stay, nursing hours and cost per case.
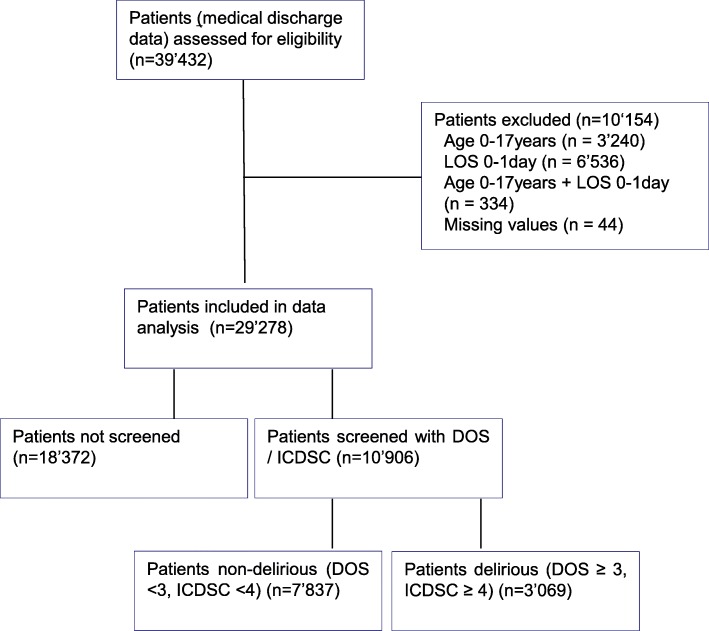
Methods: This cohort study was performed in a Swiss university hospital following implementation of a delirium management guideline. After excluding patients aged < 18 years or with a length of stay (LOS) < 1 day, 29'278 patients hospitalized in the study hospital in 2014 were included. Delirium period prevalence was calculated based on a Delirium Observation Scale (DOS) score ≥ 3 and / or Intensive Care Delirium Screening Checklist (ICDSC) scores ≥4.
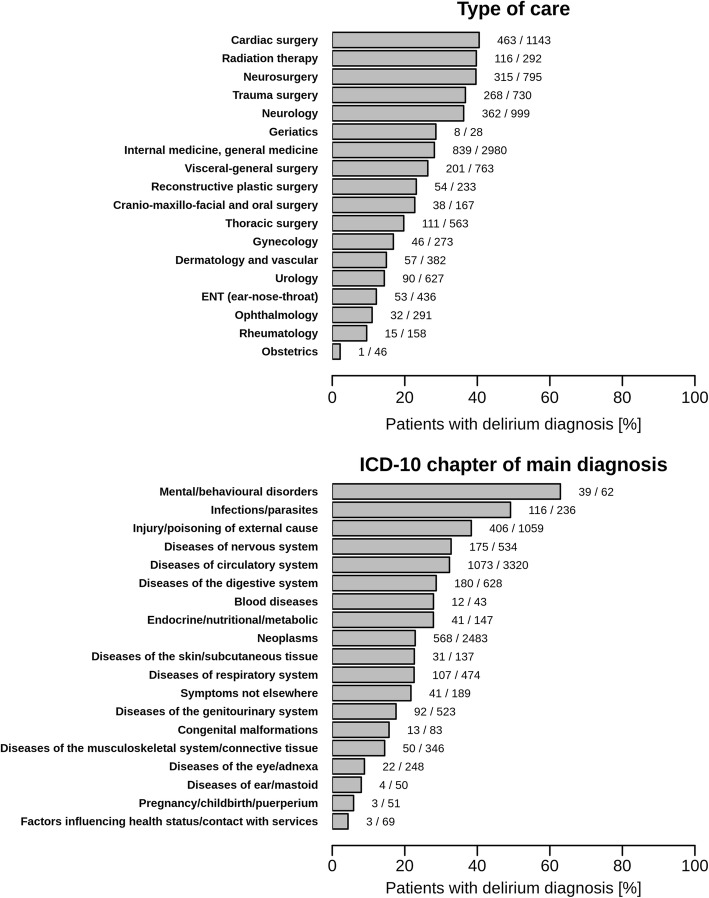
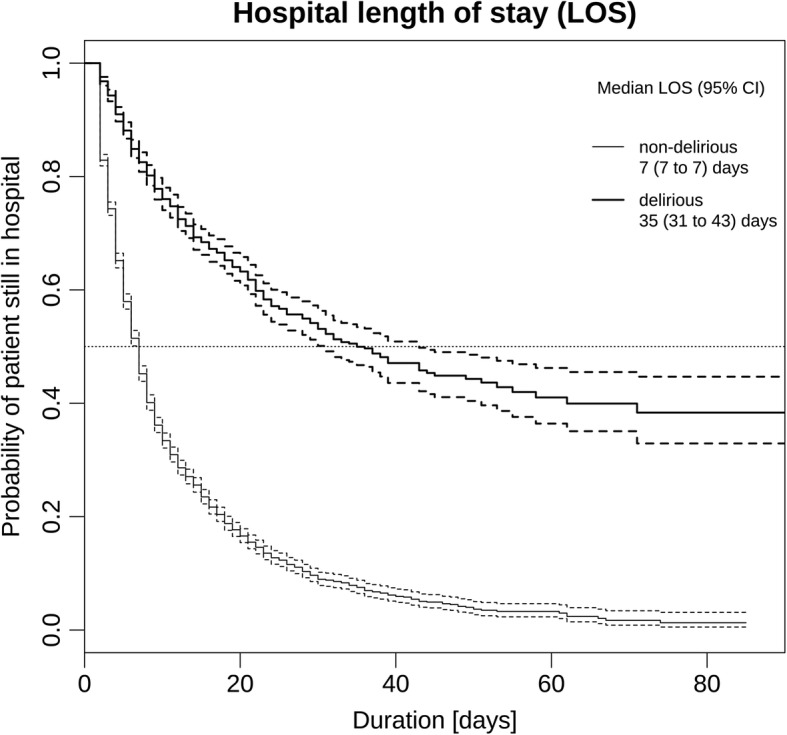
Results: Of 10'906 patients admitted, DOS / ICDSC scores indicated delirium in 28.4%. Delirium was most prevalent (36.2-40.5%) in cardiac surgery, neurosurgery, trauma, radiotherapy and neurology patients. It was also common in geriatrics, internal medicine, visceral surgery, reconstructive plastic surgery and cranio-maxillo-facial surgery patients (prevalence 21.6-28.6%). In the unadjusted and adjusted models, delirious patients had a significantly higher risk of inpatient mortality, stayed significantly longer in the ICU and hospital, needed significantly more nursing hours and generated significantly higher costs per case. For the seven most common ICD-10 diagnoses, each diagnostic group's delirious patients had worse outcomes compared to those with no delirium.
Conclusions: The results indicate a high number of patients at risk for delirium, with high delirium prevalence across all patient groups. Delirious patients showed significantly worse clinical outcomes and generated higher costs. Subgroup analyses highlighted striking variations in delirium period-prevalence across patient groups. Due to the high prevalence of delirium in patients treated in care centers for radiotherapy, visceral surgery, reconstructive plastic surgery, cranio-maxillofacial surgery and oral surgery, it is recommended to expand the current focus of delirium management to these patient groups.
Keywords: Cost of diseases OR economic burden of diseases; Delirium; Hospital mortality; Length of stay; Neurocognitive disorders.
Conflict of interest statement
Ethics approval and consent to participate
This study (PB_2016–01264) was approved by the responsible ethics board of the Kantonale Ethikkommission des Kanton Zurich and carried out in accordance with the Declaration of Helsinki, taking into consideration local regulations and standards.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Meagher DJ, Morandi A, Inouye SK, Ely W, Adamis D, Maclullich AJ, Rudolph JL, Neufeld K, Leonard M, Bellelli G, et al. Concordance between DSM-IV and DSM-5 criteria for delirium diagnosis in a pooled database of 768 prospectively evaluated patients using the delirium rating scale-revised-98. BMC Med. 2014;12:164. doi: 10.1186/s12916-014-0164-8. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
