

Repeated vital sign measurements in the emergency department predict patient deterioration within 72 hours: a prospective observational study
- PMID: 30005671
- PMCID: PMC6045840
- DOI: 10.1186/s13049-018-0525-y
Repeated vital sign measurements in the emergency department predict patient deterioration within 72 hours: a prospective observational study
Abstract
Background: More than one in five patients presenting to the emergency department (ED) with (suspected) infection or sepsis deteriorate within 72 h from admission. Surprisingly little is known about vital signs in relation to deterioration, especially in the ED. The aim of our study was to determine whether repeated vital sign measurements in the ED can differentiate between patients who will deteriorate within 72 h and patients who will not deteriorate.
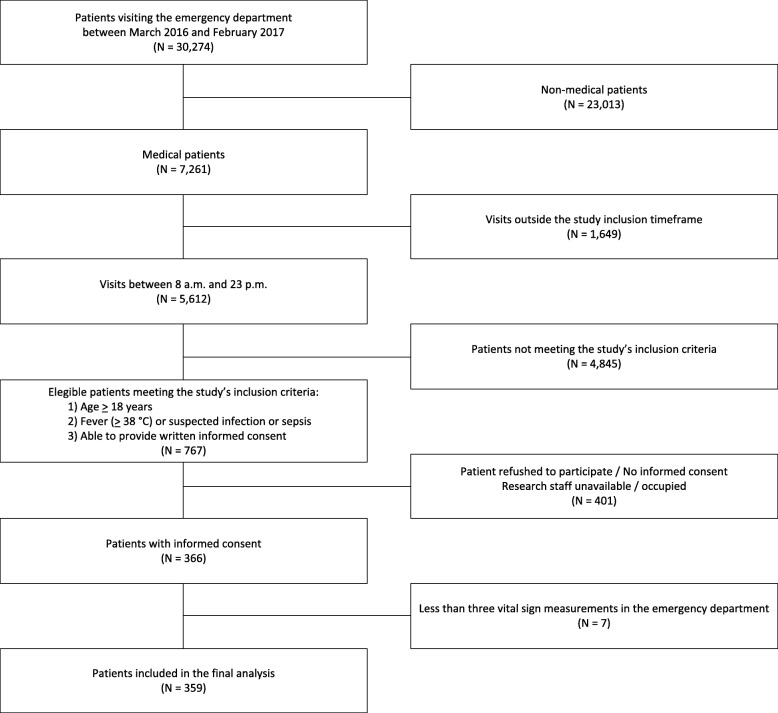
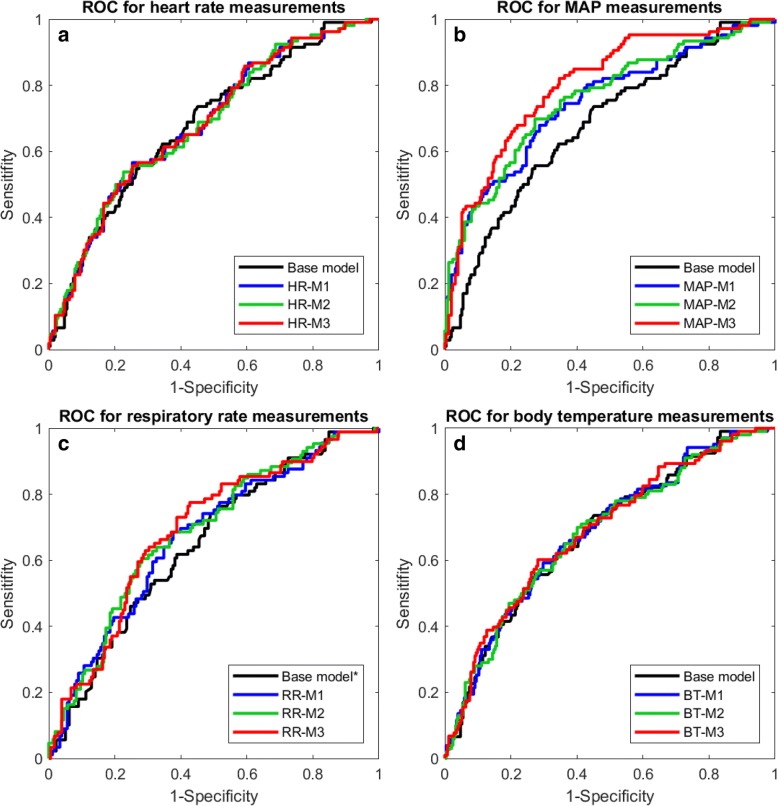
Methods: We performed a prospective observational study in patients presenting with (suspected) infection or sepsis to the ED of our tertiary care teaching hospital. Vital signs (heart rate, mean arterial pressure (MAP), respiratory rate and body temperature) were measured in 30-min intervals during the first 3 h in the ED. Primary outcome was patient deterioration within 72 h from admission, defined as the development of acute kidney injury, liver failure, respiratory failure, intensive care unit admission or in-hospital mortality. We performed a logistic regression analysis using a base model including age, gender and comorbidities. Thereafter, we performed separate logistic regression analyses for each vital sign using the value at admission, the change over time and its variability. For each analysis, the odds ratios (OR) and area under the receiver operator curve (AUC) were calculated.
Results: In total 106 (29.5%) of the 359 patients deteriorated within 72 h from admission. Within this timeframe, 18.3% of the patients with infection and 32.9% of the patients with sepsis at ED presentation deteriorated. Associated with deterioration were: age (OR: 1.02), history of diabetes (OR: 1.90), heart rate (OR: 1.01), MAP (OR: 0.96) and respiratory rate (OR: 1.05) at admission, changes over time of MAP (OR: 1.04) and respiratory rate (OR: 1.44) as well as the variability of the MAP (OR: 1.06). Repeated measurements of heart rate and body temperature were not associated with deterioration.
Conclusions: Repeated vital sign measurements in the ED are better at identifying patients at risk for deterioration within 72 h from admission than single vital sign measurements at ED admission.
Keywords: Accident & emergency medicine; Patient deterioration; Sepsis; Vital signs.
Conflict of interest statement
Ethics approval and consent to participate
This study was carried out in accordance to the Declaration of Helsinki, the Dutch Agreement on Medical Treatment Act and the Dutch Personal Data Protection Act. The Institutional Review Board of the University Medical Center Groningen ruled that the Dutch Medical Research Involving Human Subjects Act is not applicable for this study and granted a waiver (METc 2015/164). All participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Quinten VM, van Meurs M, Renes MH, Ligtenberg JJM, ter Maaten JC. Protocol of the SepsiVit study: a prospective observational study to determine whether continuous heart rate variability measurement during the first 48 hours of hospitalization provides an early warning for deterioration in patients presenting with infec. BMJ Open [Internet]. British Medical Journal Publishing Group; 2017 [cited 2017 Nov 20];7:1–17. Available from: http://www.ncbi.nlm.nih.gov/pubmed/29151053 - PMC - PubMed
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. [Internet]. Springer Berlin Heidelberg; 2017;43:304–377. Available from: https://link.springer.com/article/10.1007/s00134-017-4683-6 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
