

Fixation instability during binocular viewing in anisometropic and strabismic children
- PMID: 30006273
- PMCID: PMC7323568
- DOI: 10.1016/j.exer.2018.07.013
Fixation instability during binocular viewing in anisometropic and strabismic children
Abstract
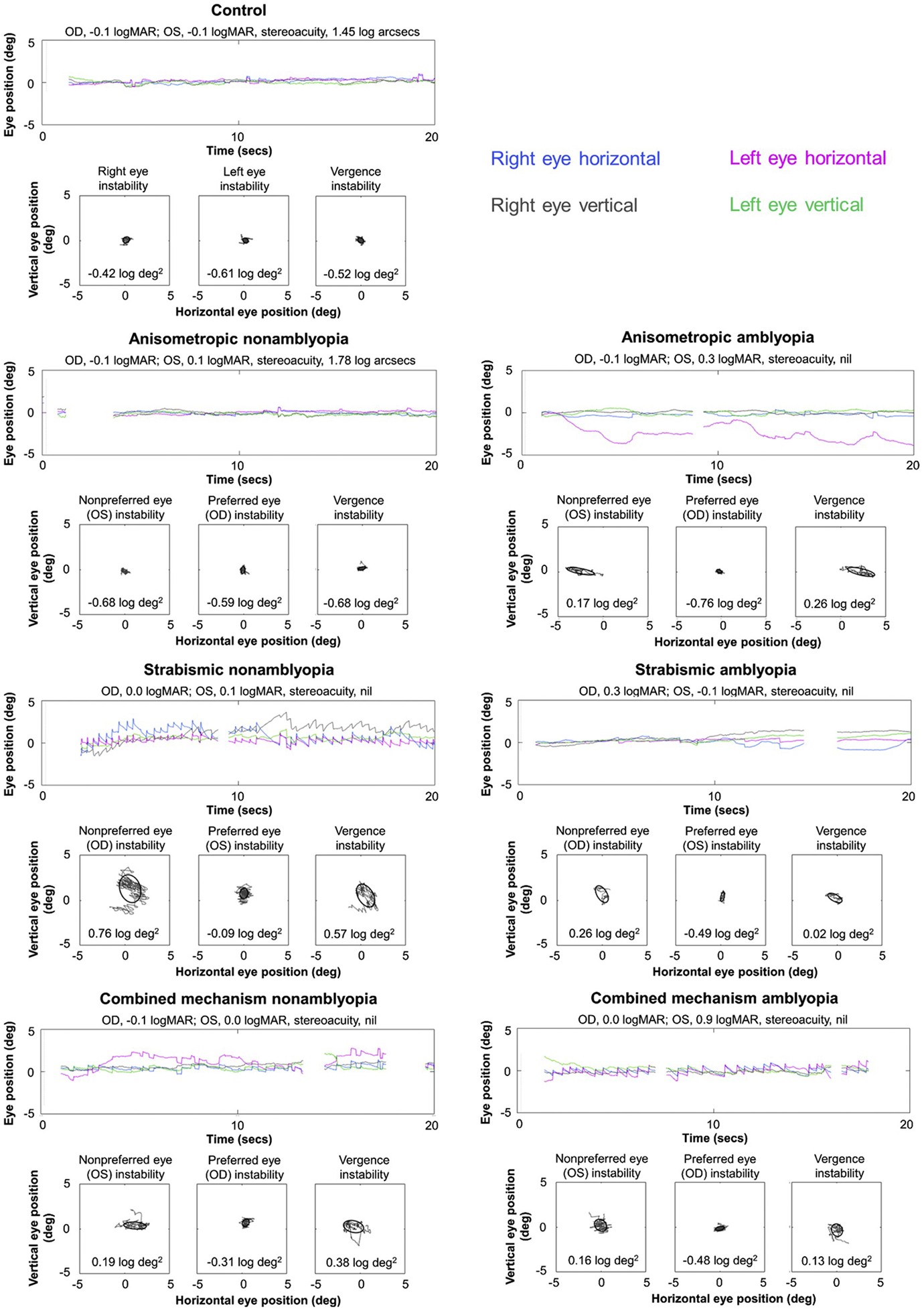
Purpose: Strabismus or anisometropia disrupts binocularity and results in fixation instability, which is increased with amblyopia. Fixation instability has typically been assessed for each eye individually. Recently, vergence instability was reported in exotropic adults and monkeys during binocular viewing. We evaluated fixation instability during binocular viewing in children treated for anisometropia and/or strabismus.
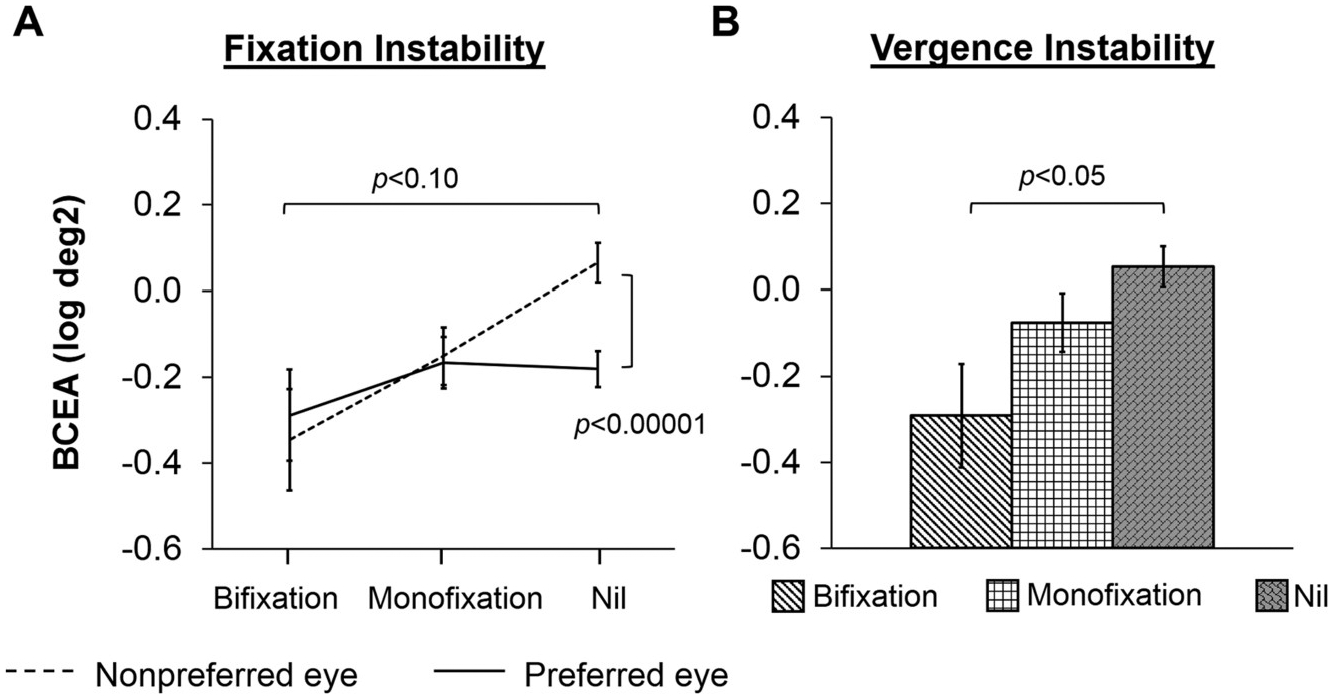
Methods: 160 children age 4-12 years with treated esotropia and/or anisometropia (98 amblyopic, 62 nonamblyopic) were compared to 46 age-similar controls. Fixation instability was recorded during binocular fixation of a 0.3 deg diameter dot for 20 s using a 500 Hz remote video binocular eye tracker (EyeLink 1000; SR Research). The bivariate contour ellipse area (BCEA; log deg2) for fixation instability was calculated for each eye (nonpreferred, preferred) and for vergence instability (left eye position - right eye position). Best-corrected visual acuity, Randot Preschool stereoacuity, and extent of suppression scotoma (Worth 4-Dot) were also obtained.
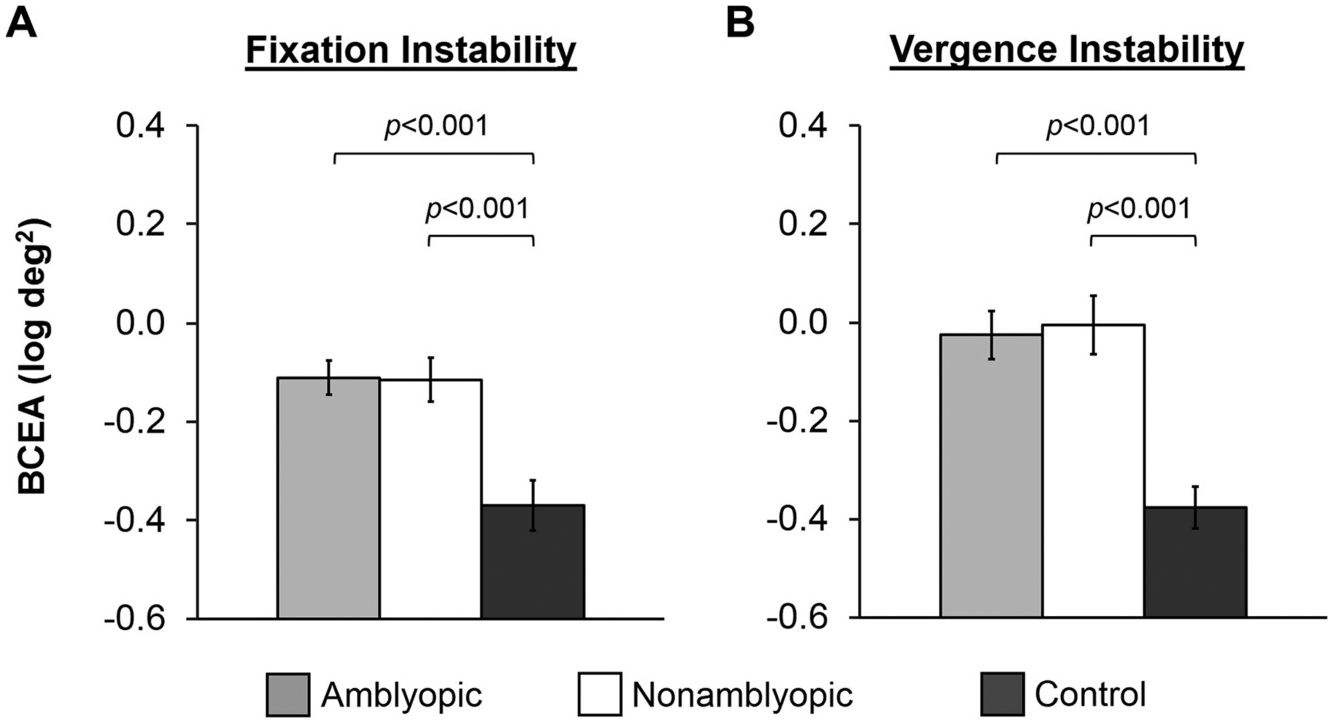
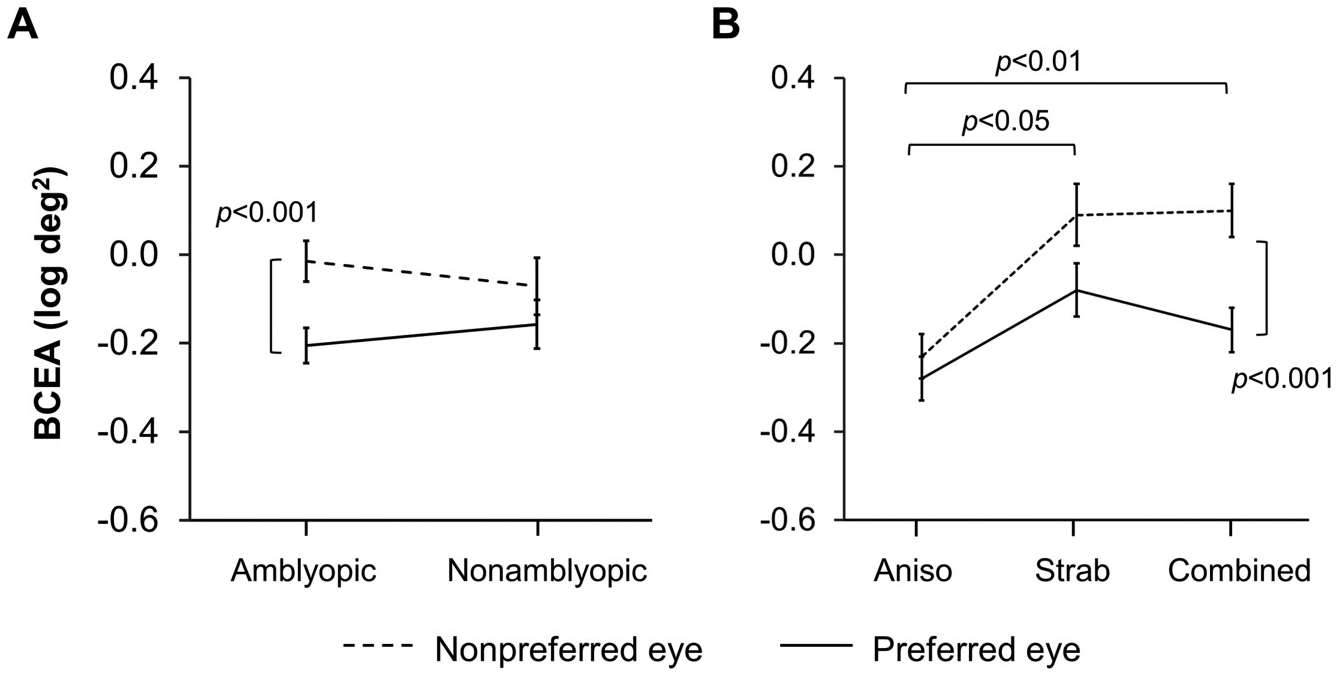
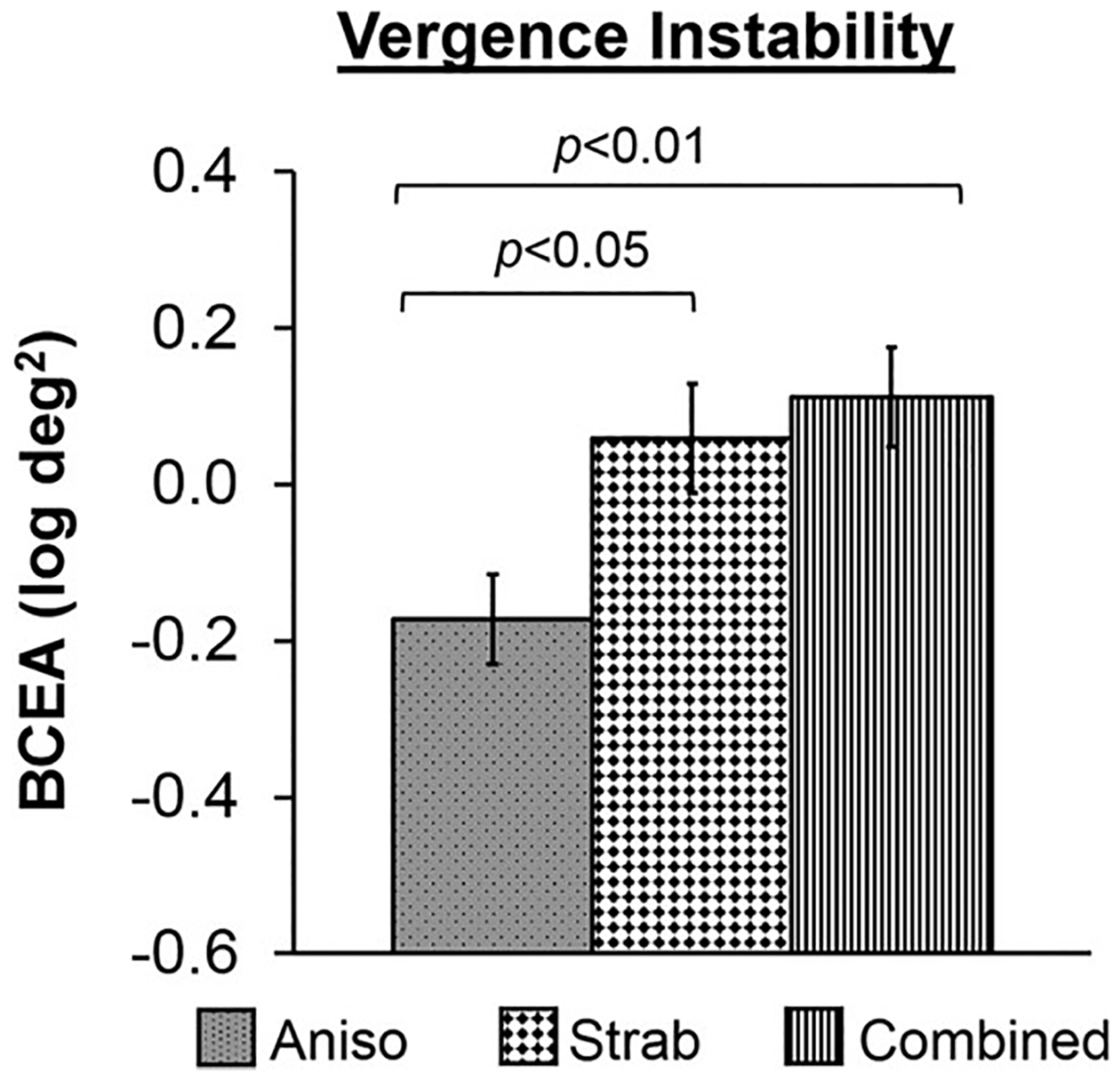
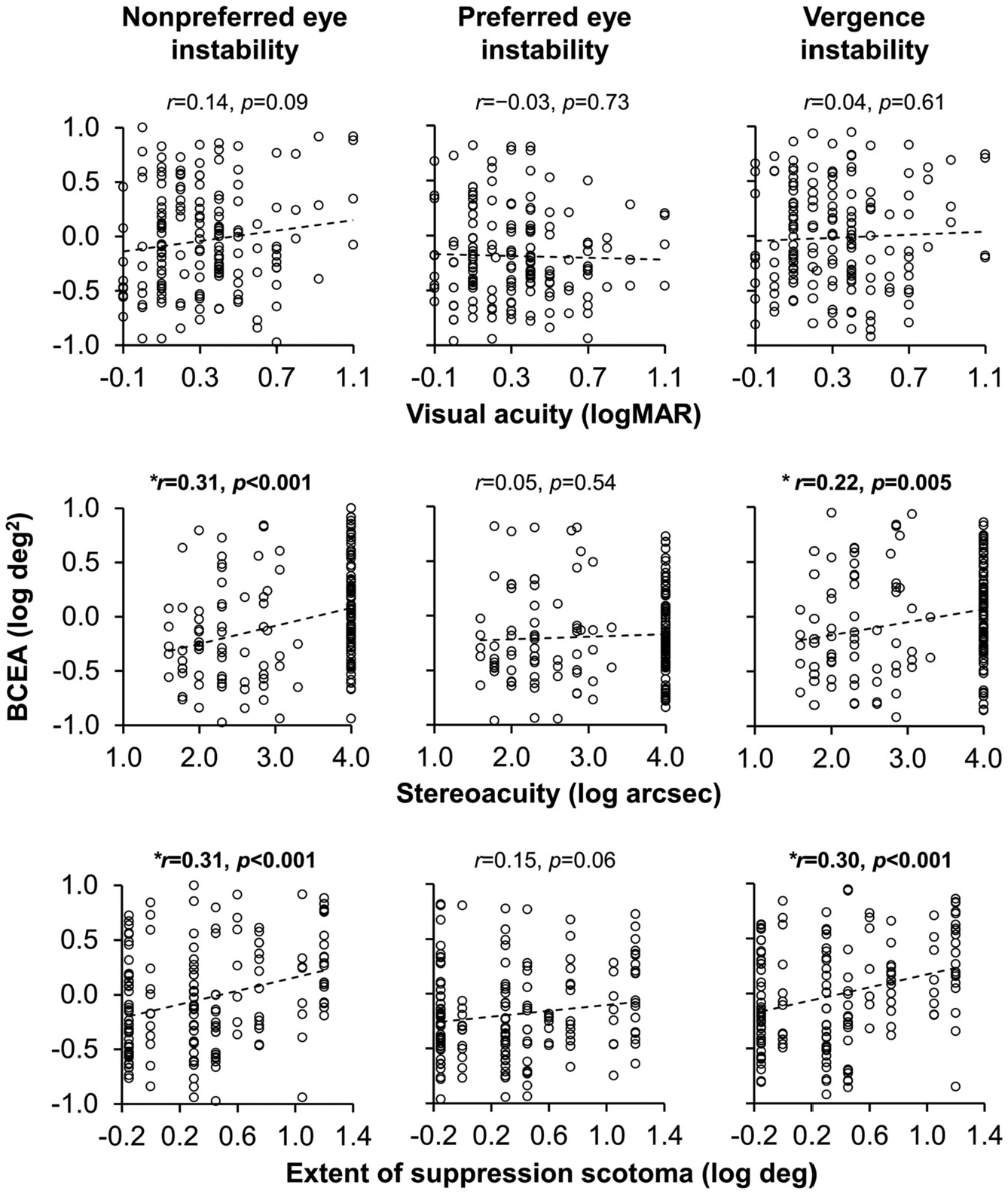
Results: When binocularly viewing, both amblyopic and nonamblyopic children treated for anisometropia and/or strabismus had larger fixation instability and vergence instability than controls. Amblyopia primarily added to the instability of the nonpreferred eye. Anisometropic children had less nonpreferred eye instability and vergence instability than those with strabismus or combined mechanism. Nonpreferred eye instability and vergence instability were related to poorer stereoacuity and a larger suppression scotoma. Preferred eye instability was not related to any visual outcome measure. No relationships were found with visual acuity.
Conclusions: Fixation instability and vergence instability during binocular viewing suggests that discordant binocular visual experience during childhood, especially strabismus, interferes with ocular motor development. Amblyopia adds to instability of the nonpreferred eye. Vergence instability may limit potential for recovery of binocular vision in these children.
Keywords: Amblyopia; Anisometropia; Fixation instability; Ocular motor development; Strabismus; Vergence.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflicts of interest
None of the authors have a financial conflict of interest with any of the material presented in the manuscript. This work was supported by the National Eye Institute (EY02313 and K99EY028224).
Figures
References
-
- Beck R, Moke P, Turpin A, et al. , 2003. A computerized method of visual acuity testing: adaptation of the early treatment of diabetic retinopathy study testing protocol. Am. J. Ophthalmol 135 (2), 194–205. - PubMed
-
- Birch EE, 2003. Marshall Parks lecture. Binocular sensory outcomes in accommodative ET. J AAPOS 7 (6), 369–373. - PubMed
-
- Birch EE, Stager DR, 2006. Long-term motor and sensory outcomes after early surgery for infantile esotropia. J AAPOS 10 (5), 409–413. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
