

Using Mobile Health to Enhance Outcomes of Noncommunicable Diseases Care in Rural Settings and Refugee Camps: Randomized Controlled Trial
- PMID: 30006326
- PMCID: PMC6064041
- DOI: 10.2196/mhealth.8146
Using Mobile Health to Enhance Outcomes of Noncommunicable Diseases Care in Rural Settings and Refugee Camps: Randomized Controlled Trial
Abstract
Background: Rural areas and refugee camps are characterized by poor access of patients to needed noncommunicable disease (NCD)-related health services, including diabetes and hypertension. Employing low-cost innovative eHealth interventions, such as mobile health (mHealth), may help improve NCDs prevention and control among disadvantaged populations.
Objective: The aim of this study was to assess the effect of employing low-cost mHealth tools on the accessibility to health services and improvement of health indicators of individuals with NCDs in rural areas and refugee camps in Lebanon.
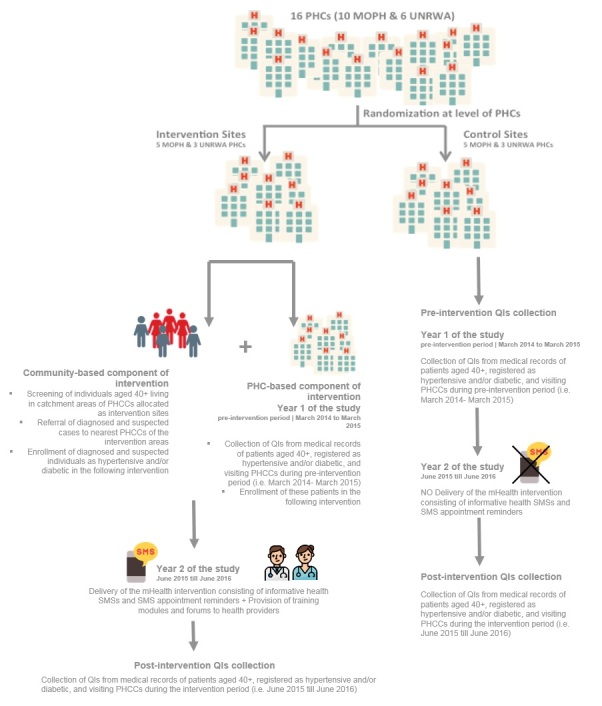
Methods: This is a randomized controlled trial study in which centers were allocated randomly into control and intervention sites. The effect of an employed mHealth intervention is assessed through selected quality indicators examined in both control and intervention groups. Sixteen primary health care centers (eight controls, eight interventions) located in rural areas and Palestinian refugee camps across Lebanon were included in this study. Data on diabetic and hypertensive patients-1433 in the intervention group and 926 in the control group-was extracted from patient files in the pre and postintervention periods. The intervention entailed weekly short message service messages, including medical information, importance of compliance, and reminders of appointments or regular physician follow-up. Internationally established care indicators were utilized in this study. Descriptive analysis of baseline characteristics of participants, bivariate analysis, logistic and linear regression were conducted using SPSS (IBM Corp).
Results: Bivariate analysis of quality indicators indicated that the intervention group had a significant increase in blood pressure control (P=.03), as well as a significant decrease in the mean systolic blood pressure (P=.02), mean glycated hemoglobin (HbA1c; P<.01), and in the proportion of HbA1c poor control (P=.02). Separate regression models controlling for age, gender, and setting showed a 28% increase in the odds of blood pressure control (P=.05) and a 38% decrease in the odds of HbA1c poor control (P=.04) among the intervention group in the posttest period. Females were at lower odds of HbA1c poor control (P=.01), and age was statistically associated with annual HbA1c testing (P<.01). Regression models for mean systolic blood pressure, mean diastolic blood pressure, and mean HbA1c showed that a mean decrease in HbA1c of 0.87% (P<.01) pretest to posttest period was observed among the intervention group. Patients in rural areas belonging to the intervention group had a lower HbA1c score as compared with those in refugee camps (P<.01).
Conclusions: This study underlines the importance of employing integrative approaches of diseases prevention and control in which existing NCD programs in underserved communities (ie, rural and refugee camps settings) are coupled with innovative, low-cost approaches such as mHealth to provide an effective and amplified effect of traditional NCD-targeted care that can be reflected by improved NCD-related health indicators among the population.
Trial registration: ClinicalTrials.gov NCT03580330; https://clinicaltrials.gov/ct2/show/NCT03580330 (Archived by WebCite at http://www.webcitation.org/70mhVEUwQ).
Keywords: diabetes mellitus; hypertension; mobile health; noncommunicable diseases; refugees; rural health; telemedicine.
©Shadi Saleh, Angie Farah, Hani Dimassi, Nour El Arnaout, Joanne Constantin, Mona Osman, Christo El Morr, Mohamad Alameddine. Originally published in JMIR Mhealth and Uhealth (http://mhealth.jmir.org), 13.07.2018.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- World Health Organization. 2012. The top 10 causes of death http://www.who.int/en/news-room/fact-sheets/detail/the-top-10-causes-of-... .
-
- World Health Organization. 2015. NCD mortality and morbidity, Global Health Observatory (GHO) data http://www.who.int/gho/ncd/mortality_morbidity/en/
-
- The PLoS Medicine Editors Addressing global disparities in the burden of noncommunicable diseases: call for papers. PLoS Med. 2012 Dec 27;9(12):e1001360. doi: 10.1371/journal.pmed.1001360. - DOI
-
- Reddy KS. Cardiovascular diseases in the developing countries: dimensions, determinants, dynamics, and directions for public health action. Public Health Nutr. 2002 Feb;5(1A):231–7.S1368980002000320 - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
