

Acute Declines in Renal Function during Intensive BP Lowering and Long-Term Risk of Death
- PMID: 30006417
- PMCID: PMC6115661
- DOI: 10.1681/ASN.2018040365
Acute Declines in Renal Function during Intensive BP Lowering and Long-Term Risk of Death
Abstract
Background: During intensive BP lowering, acute declines in renal function are common, thought to be hemodynamic, and potentially reversible. We previously showed that acute declines in renal function ≥20% during intensive BP lowering were associated with higher risk of ESRD. Here, we determined whether acute declines in renal function during intensive BP lowering were associated with mortality risk among 1660 participants of the African American Study of Kidney Disease and Hypertension and the Modification of Diet in Renal Disease Trial.
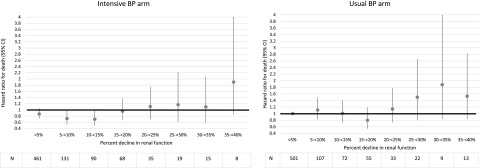
Methods: We used Cox models to examine the association between percentage decline in eGFR (<5%, 5% to <20%, or ≥20%) between randomization and months 3-4 of the trials (period of therapy intensification) and death.
Results: In adjusted analyses, compared with a <5% eGFR decline in the usual BP arm (reference), a 5% to <20% eGFR decline in the intensive BP arm was associated with a survival benefit (hazard ratio [HR], 0.77; 95% confidence interval [95% CI], 0.62 to 0.96), but a 5% to <20% eGFR decline in the usual BP arm was not (HR, 1.01; 95% CI, 0.81 to 1.26; P<0.05 for the interaction between intensive and usual BP arms for mortality risk). A ≥20% eGFR decline was not associated with risk of death in the intensive BP arm (HR, 1.18; 95% CI, 0.86 to 1.62), but it was associated with a higher risk of death in the usual BP arm (HR, 1.40; 95% CI, 1.04 to 1.89) compared with the reference group.
Conclusions: Intensive BP lowering was associated with a mortality benefit only if declines in eGFR were <20%.
Keywords: AASK (African American Study of Kidney Disease and Hypertension); chronic renal disease; hypertension; mortality risk.
Copyright © 2018 by the American Society of Nephrology.
Figures
References
-
- Holtkamp FA, de Zeeuw D, Thomas MC, Cooper ME, de Graeff PA, Hillege HJ, et al.: An acute fall in estimated glomerular filtration rate during treatment with losartan predicts a slower decrease in long-term renal function. Kidney Int 80: 282–287, 2011 - PubMed
-
- Christensen PK, Hansen HP, Parving HH: Impaired autoregulation of GFR in hypertensive non-insulin dependent diabetic patients. Kidney Int 52: 1369–1374, 1997 - PubMed
-
- Anonymous: Short-term effects of protein intake, blood pressure, and antihypertensive therapy on glomerular filtration rate in the Modification of Diet in Renal Disease study. J Am Soc Nephrol 7: 2097–2109, 1996 - PubMed
-
- Palmer BF: Renal dysfunction complicating the treatment of hypertension. N Engl J Med 347: 1256–1261, 2002 - PubMed
-
- Anderson S, Brenner BM: Intraglomerular hypertension: Implications and drug treatment. Annu Rev Med 39: 243–253, 1988 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
