

Practice Guideline
doi: 10.6004/jnccn.2018.0060.
Anal Carcinoma, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology
- PMID: 30006428
- PMCID: PMC10181270
- DOI: 10.6004/jnccn.2018.0060
Item in Clipboard
Practice Guideline
Anal Carcinoma, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology
J Natl Compr Canc Netw.
2018 Jul.
Abstract
The NCCN Guidelines for Anal Carcinoma provide recommendations for the management of patients with squamous cell carcinoma of the anal canal or perianal region. Primary treatment of anal cancer usually includes chemoradiation, although certain lesions can be treated with margin-negative local excision alone. Disease surveillance is recommended for all patients with anal carcinoma because additional curative-intent treatment is possible. A multidisciplinary approach including physicians from gastroenterology, medical oncology, surgical oncology, radiation oncology, and radiology is essential for optimal patient care.
Copyright © 2018 by the National Comprehensive Cancer Network.
Figures
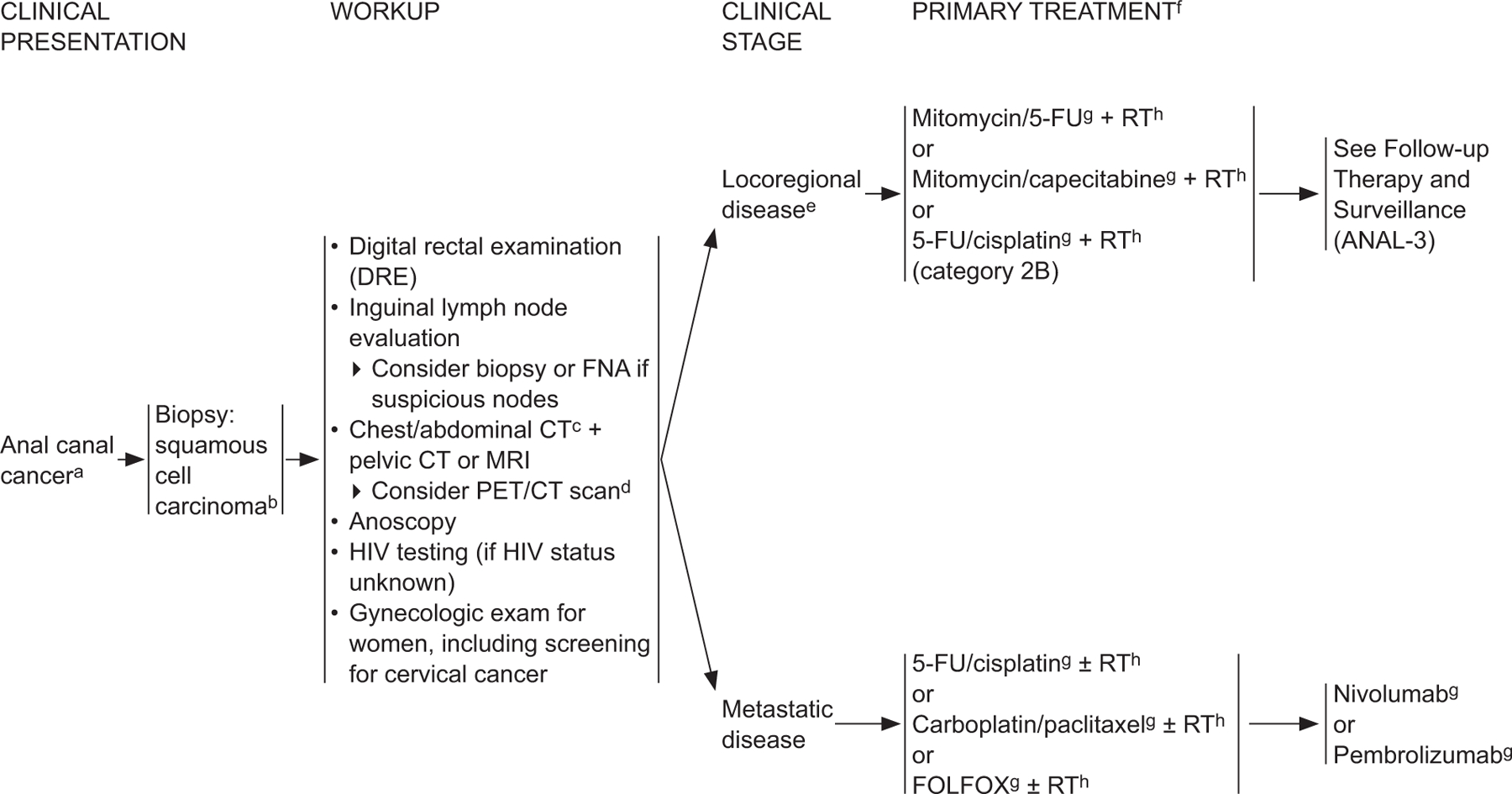
ANAL-1 aThe superior border of the functional anal canal, separating it from the rectum, has been defined as the palpable upper border of the anal sphincter and puborectalis muscles of the anorectal ring. It is approximately 3 to 5 cm in length, and its inferior border starts at the anal verge, the lowermost edge of the sphincter muscles, corresponding to the introitus of the anal orifice. bFor melanoma histology, see the NCCN Guidelines for Melanoma*; for adenocarcinoma, see the NCCN Guidelines for Rectal Cancer (elsewhere in this issue). cCT should be with IV and oral contrast. Pelvic MRI with contrast. dPET/CT scan does not replace a diagnostic CT. PET/CT performed skull base to mid-thigh. eSee Principles of Surgery (ANAL-A†). fModifications to cancer treatment should not be made solely on the basis of HIV status. See NCCN Guidelines for Cancer in People Living with HIV*. gSee Principles of Chemotherapy (ANAL-B†). hSee Principles of Radiation Therapy (ANAL-C†). *To view the most recent version of these guidelines, visit NCCN.org . †Available online, in these guidelines, at NCCN.org .
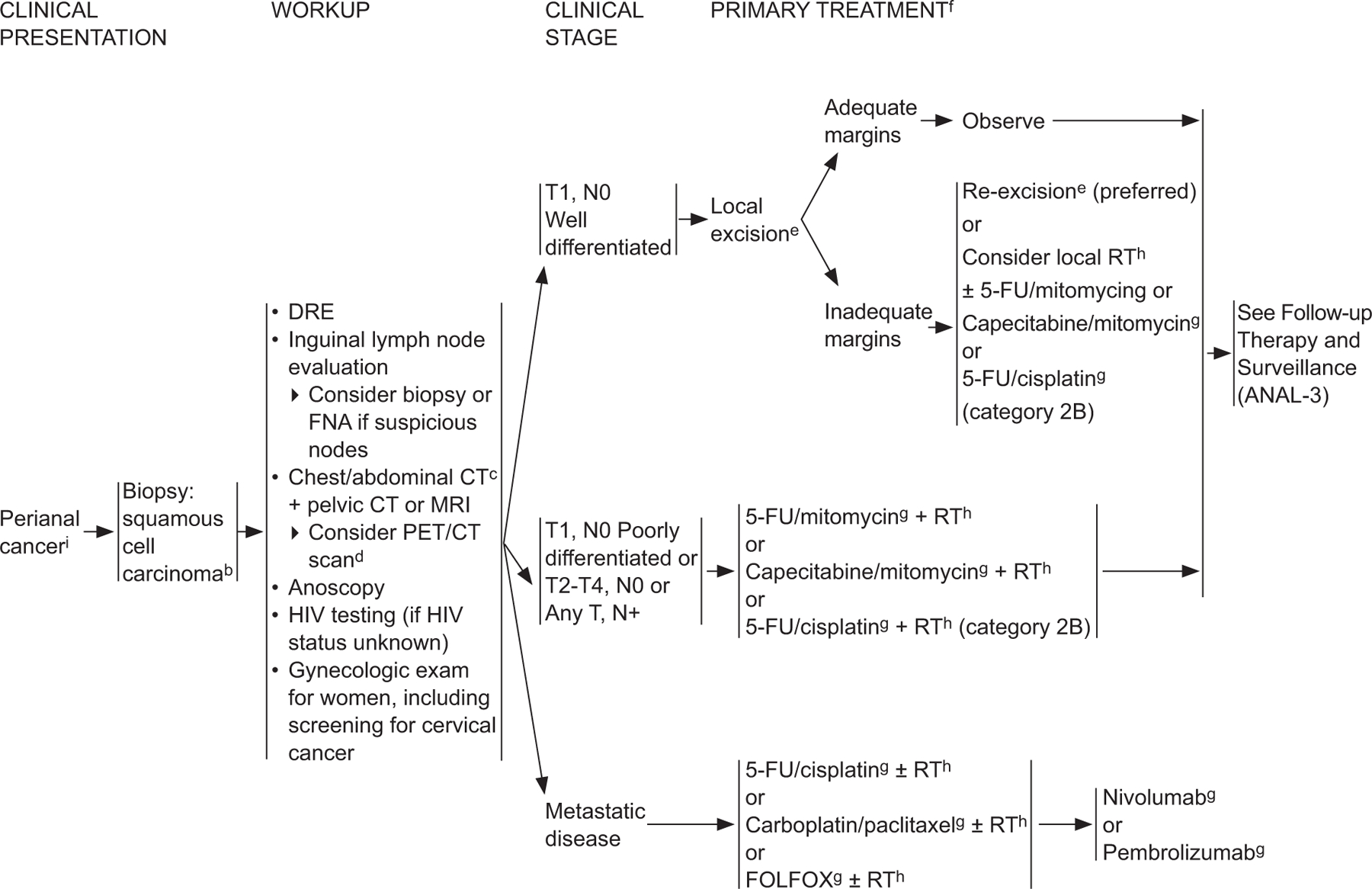
ANAL-2 bFor melanoma histology, see the NCCN Guidelines for Melanoma*; for adenocarcinoma, see the NCCN Guidelines for Rectal Cancer (elsewhere in this issue). cCT should be with IV and oral contrast. Pelvic MRI with contrast. dPET/CT scan does not replace a diagnostic CT. PET/CT performed skull base to mid-thigh. eSee Principles of Surgery (ANAL-A†). fModifications to cancer treatment should not be made solely on the basis of HIV status. gSee Principles of Chemotherapy (ANAL-B†). hSee Principles of Radiation Therapy (ANAL-C†). iThe perianal region starts at the anal verge and includes the perianal skin over a 5-cm radius from the squamous mucocutaneous junction. *To view the most recent version of these guidelines, visit NCCN.org . †Available online, in these guidelines, at NCCN.org .
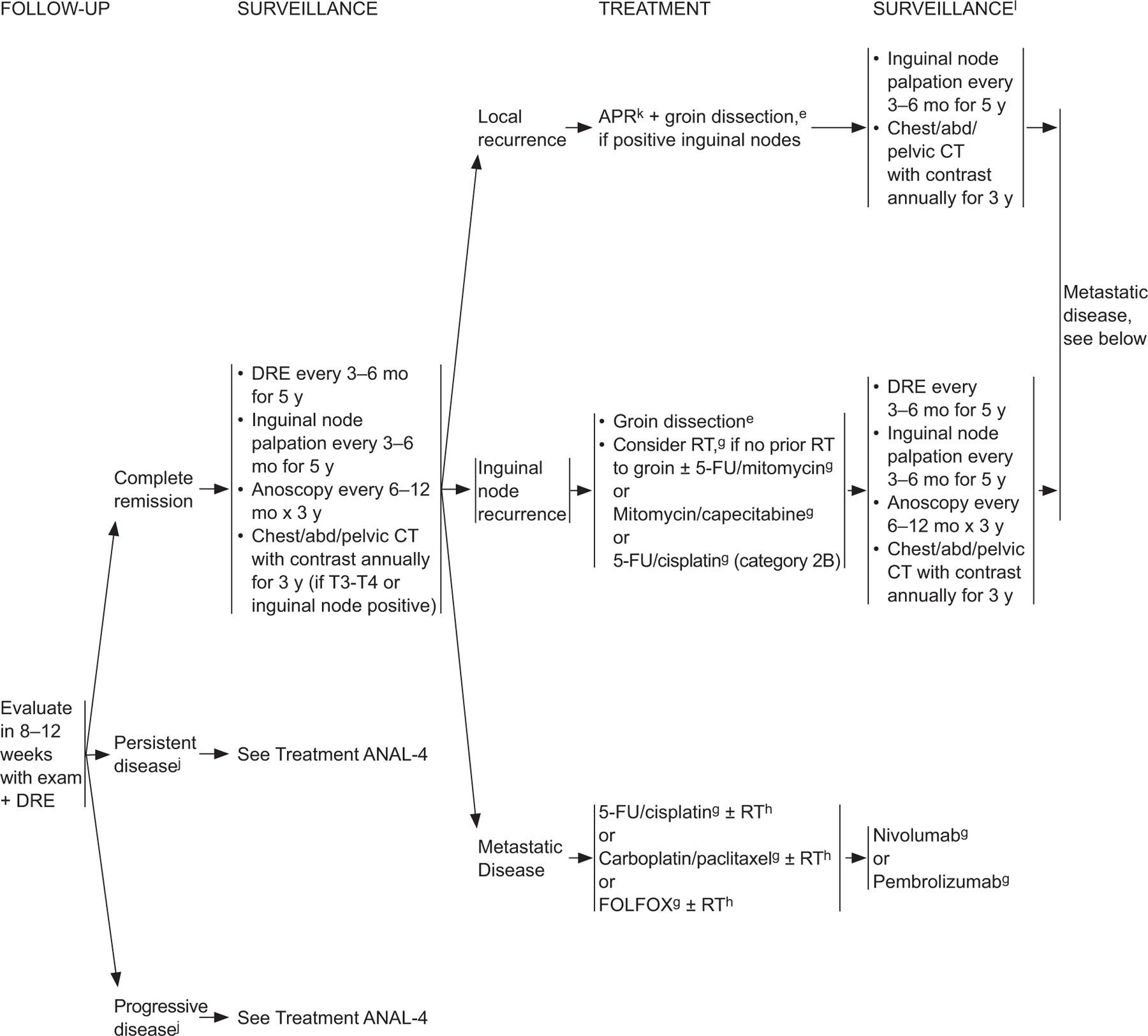
ANAL-3 eSee Principles of Surgery (ANAL-A†). gSee Principles of Chemotherapy (ANAL-B†). hSee Principles of Radiation Therapy (ANAL-C†). jBased on the results of the ACT-II study, it may be appropriate to follow patients who have not achieved a complete clinical response with persistent anal cancer up to 6 months following completion of radiation therapy and chemotherapy as long as there is no evidence of progressive disease during this period of follow-up. Persistent disease may continue to regress even at 26 weeks from the start of treatment. James RD, Glynne-Jones R, Meadows HM, et al. Mitomycin or cisplatin chemoradiation with or without maintenance chemotherapy for treatment of squamous cell carcinoma of the anus (Act II): a randomised, phase 3, open-label, 2×2 factorial trial. Lancet Oncol 2013;14:516–524. kConsider muscle flap reconstruction lSee Principles of Survivorship (ANAL-D†). †Available online, in these guidelines, at NCCN.org .
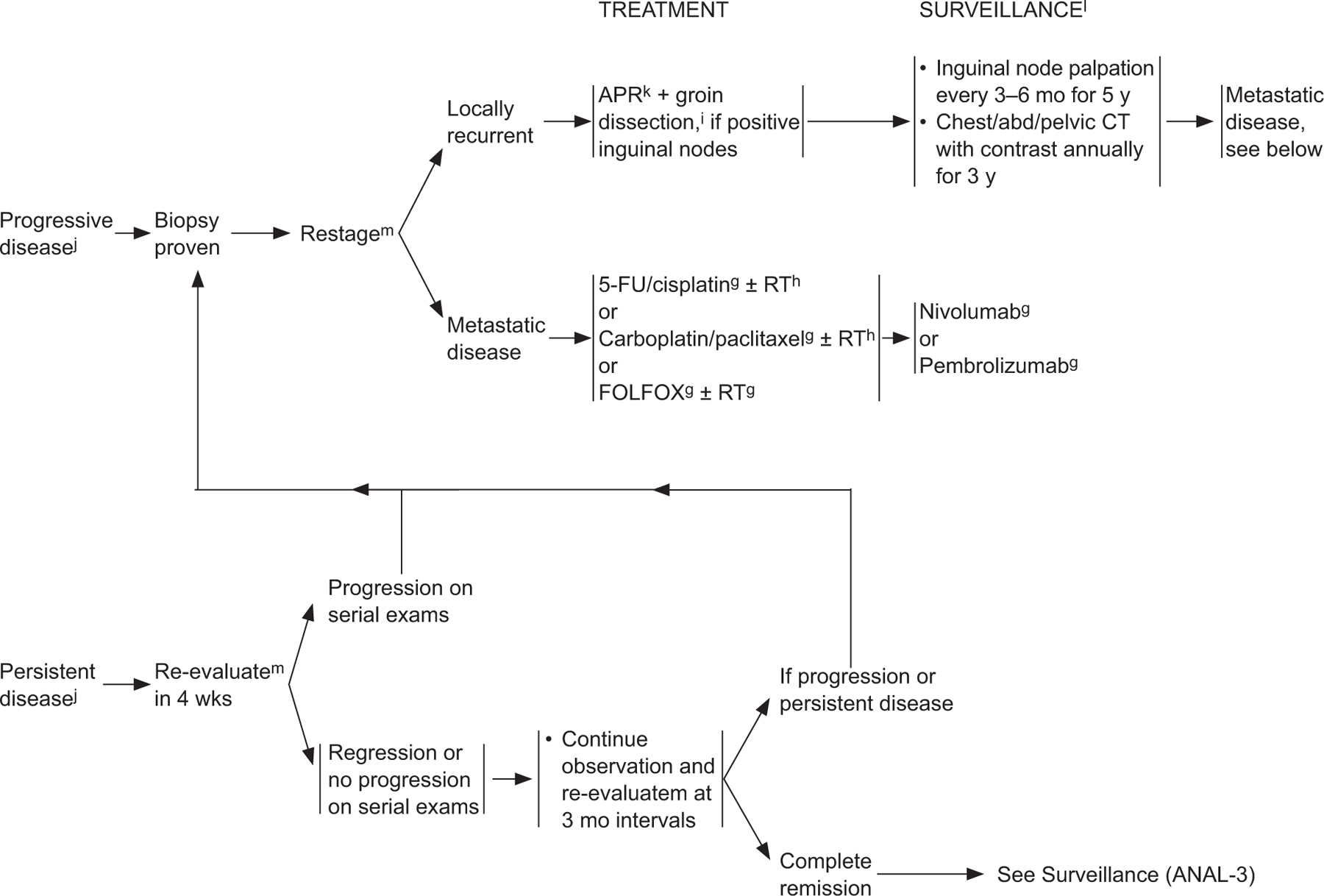
ANAL-4 gSee Principles of Chemotherapy (ANAL-B†). hSee Principles of Radiation Therapy (ANAL-C†). jBased on the results of the ACT-II study, it may be appropriate to follow patients who have not achieved a complete clinical response with persistent anal cancer up to 6 months following completion of radiation therapy and chemotherapy as long as there is no evidence of progressive disease during this period of follow-up. Persistent disease may continue to regress even at 26 weeks from the start of treatment. James RD, Glynne-Jones R, Meadows HM, et al. Mitomycin or cisplatin chemoradiation with or without maintenance chemotherapy for treatment of squamous cell carcinoma of the anus (Act II): a randomised, phase 3, open-label, 2×2 factorial trial. Lancet Oncol 2013;14:516–524. kConsider muscle flap reconstruction. lSee Principles of Survivorship (ANAL-D†) mUtilize imaging studies as per initial workup. †Available online, in these guidelines, at NCCN.org .
References
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
