

The Association of Obesity and Cardiometabolic Traits With Incident HFpEF and HFrEF
- PMID: 30007554
- PMCID: PMC6076337
- DOI: 10.1016/j.jchf.2018.05.018
The Association of Obesity and Cardiometabolic Traits With Incident HFpEF and HFrEF
Abstract
Objectives: This study evaluated the associations of obesity and cardiometabolic traits with incident heart failure with preserved versus reduced ejection fraction (HFpEF vs. HFrEF). Given known sex differences in HF subtype, we examined men and women separately.
Background: Recent studies suggest that obesity confers greater risk of HFpEF versus HFrEF. Contributions of associated metabolic traits to HFpEF are less clear.
Methods: We studied 22,681 participants from 4 community-based cohorts followed for incident HFpEF versus HFrEF (ejection fraction ≥50% vs. <50%). We evaluated the association of body mass index (BMI) and cardiometabolic traits with incident HF subtype using Cox models.
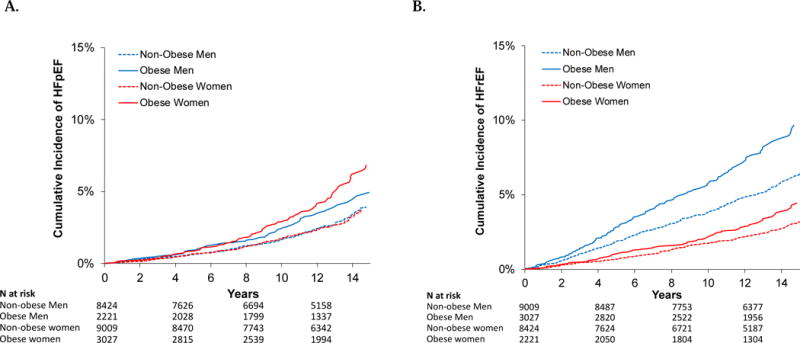
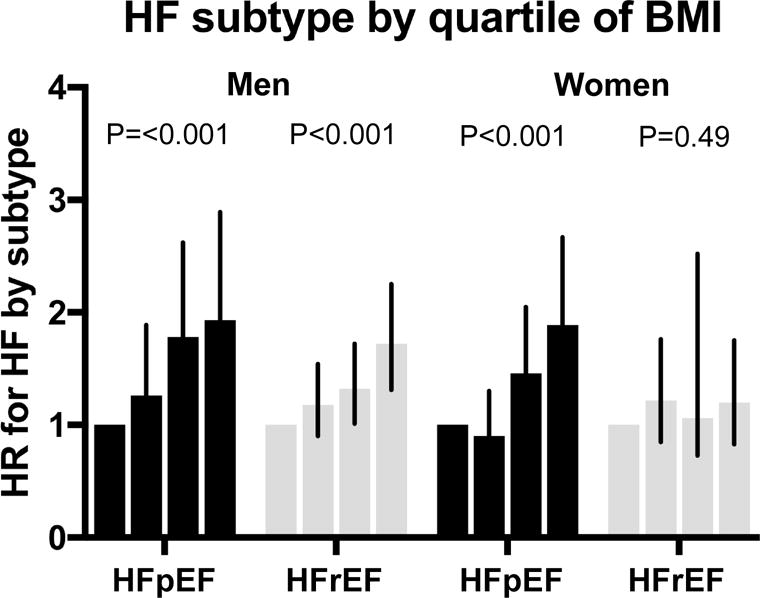
Results: The mean age was 60 ± 13 years, and 53% were women. Over a median follow-up of 12 years, 628 developed incident HFpEF and 835 HFrEF. Greater BMI portended higher risk of HFpEF compared with HFrEF (hazard ratio [HR]: 1.34 per 1-SD increase in BMI; 95% confidence interval [CI]: 1.24 to 1.45 vs. HR: 1.18; 95% CI: 1.10 to 1.27). Similarly, insulin resistance (homeostatic model assessment of insulin resistance) was associated with HFpEF (HR: 1.20 per 1-SD; 95% CI: 1.05 to 1.37), but not HFrEF (HR: 0.99; 95% CI: 0.88 to 1.11; p < 0.05 for difference HFpEF vs. HFrEF). We found that the differential association of BMI with HFpEF versus HFrEF was more pronounced among women (p for difference HFpEF vs. HFrEF = 0.01) when compared with men (p = 0.34).
Conclusions: Obesity and related cardiometabolic traits including insulin resistance are more strongly associated with risk of future HFpEF versus HFrEF. The differential risk of HFpEF with obesity seems particularly pronounced among women and may underlie sex differences in HF subtypes.
Keywords: HFpEF; heart failure; insulin resistance; obesity; sex differences.
Copyright © 2018 American College of Cardiology Foundation. All rights reserved.
Figures
Comment in
-
Fat, Female, Fatigued: Features of the Obese HFpEF Phenotype.JACC Heart Fail. 2018 Aug;6(8):710-713. doi: 10.1016/j.jchf.2018.06.006. Epub 2018 Jul 7. JACC Heart Fail. 2018. PMID: 30078394 No abstract available.
-
Obesity Is a Culprit in Heart Failure: Do NOT Miss HFpEF, Especially in Obese Women.JACC Heart Fail. 2018 Nov;6(11):971-972. doi: 10.1016/j.jchf.2018.07.011. JACC Heart Fail. 2018. PMID: 30384920 No abstract available.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2016;133:e38–360. - PubMed
-
- Bursi F, Weston SA, Redfield MM, et al. Systolic and diastolic heart failure in the community. Jama. 2006;296:2209–16. - PubMed
-
- Kenchaiah S, Evans JC, Levy D, et al. Obesity and the risk of heart failure. The New England journal of medicine. 2002;347:305–13. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- T32 HL094301/HL/NHLBI NIH HHS/United States
- N01 HC085080/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- U01 HL130114/HL/NHLBI NIH HHS/United States
- N01 HC095161/HC/NHLBI NIH HHS/United States
- N01 HC095164/HC/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- P30 DK063491/DK/NIDDK NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- HHSN268201500001I/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- K23 HL116780/HL/NHLBI NIH HHS/United States
- N01 HC095168/HC/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC085081/HL/NHLBI NIH HHS/United States
- P30 DK040561/DK/NIDDK NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- R01 HL140224/HL/NHLBI NIH HHS/United States
- N01 HC085081/HC/NHLBI NIH HHS/United States
- N01 HC095167/HC/NHLBI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC085082/HL/NHLBI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- N01 HC095166/HC/NHLBI NIH HHS/United States
- N01 HC095160/HC/NHLBI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- N01 HC095169/HC/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- K23 HL138260/HL/NHLBI NIH HHS/United States
- N01 HC095165/HC/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095163/HC/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- N01 HC085079/HC/NHLBI NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- N01 HC095162/HC/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- N01 HC095159/HC/NHLBI NIH HHS/United States
- R01 HL134893/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
