

Lumbar fusion for lytic spondylolisthesis: Is an interbody cage necessary?
- PMID: 30008528
- PMCID: PMC6024747
- DOI: 10.4103/jcvjs.JCVJS_20_18
Lumbar fusion for lytic spondylolisthesis: Is an interbody cage necessary?
Abstract
Study design: This study was a retrospective observational study.
Purpose: The purpose of the study was to determine the radiological and clinical outcome of using locally sourced autologous bone graft in the surgical management of single-level lumbar lytic spondylolisthesis.
Background: Many spinal surgeons supplement pedicle screw fixation of lumbar spondylolisthesis with cages. In developing countries, the high cost of interbody cages has precluded their use, with surgeons resorting to filling the interbody space with different types of bone graft instead. This study reports on the clinical and radiological outcome of posterior lumbar interbody fusions for low-grade lytic spondylolisthesis using locally sourced autologous bone graft.
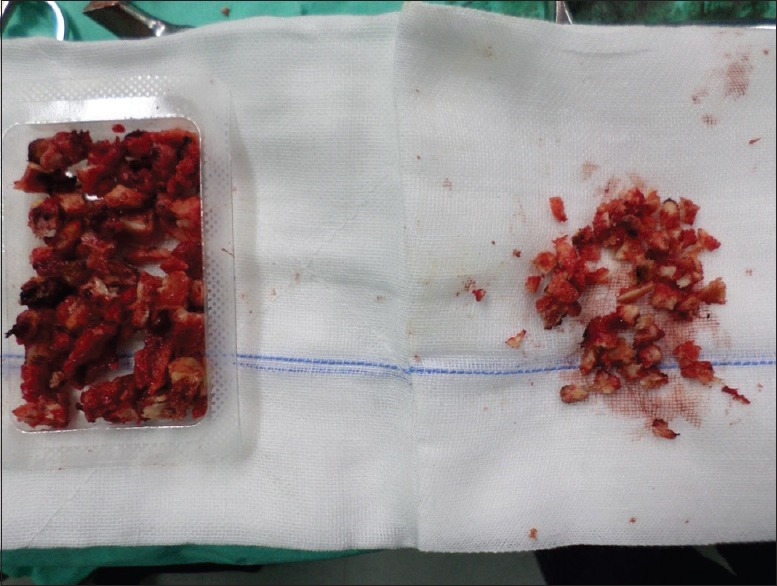
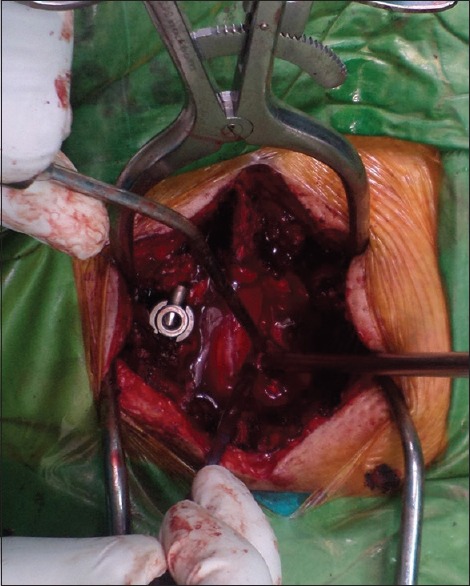
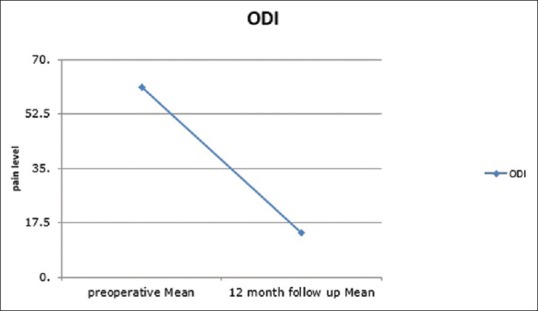
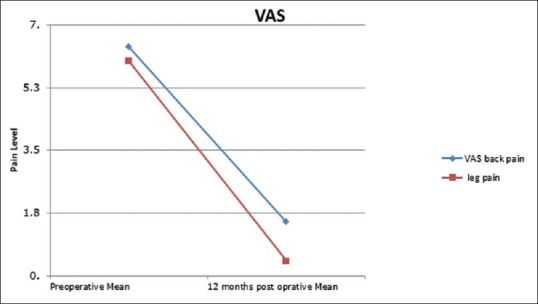
Material and methods: Posterior interbody fusion was performed in 22 consecutive patients over 18-month period, using (BRAND) pedicle screw system and locally sourced bone graft, i.e., bone removed during neural decompression. There were no postoperative restrictions, and all patients underwent clinical outcome measurements using Oswestry Disability Index (ODI), visual analogue pain score (VAS) at a minimum follow-up of 12 months, and computed tomography (CT) assessment of fusion with intraobserver validation by radiology consultant blinded, at 6 and12 months. Nearly 50% of the population were smokers.
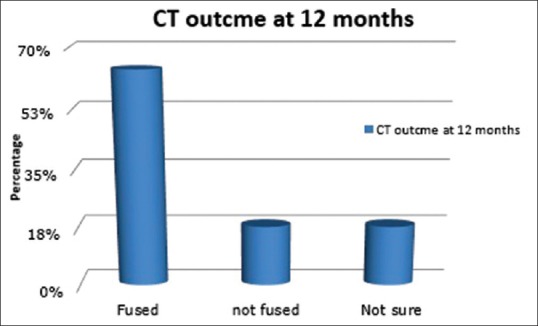
Results: There was significant clinical improvement in ODI, VAS back pain, and VAS leg pain (P < 0.001). By contrast, the radiologic fusion rate measured by CT at 12 months was less satisfactory at 64%. There was no difference in clinical outcome between the fused group and nonfused population.
Conclusions: These results indicate that the use of locally sourced bone graft in single-level lumbar lytic low-grade spondylolisthesis. Interbody fusion provides good clinical outcomes. The use of an interbody cage may not be clinically necessary. Our radiologic outcome, however, shows inferior fusion rates compared with published data. Future research will focus on long-term outcomes.
Keywords: Back pain; interbody cage; lumbar fusion; lumbar spine; lytic spondylolisthesis.
Conflict of interest statement
There are no conflicts of interest.
Figures

References
-
- Ha KY, Na KH, Shin JH, Kim KW. Comparison of posterolateral fusion with and without additional posterior lumbar interbody fusion for degenerative lumbar spondylolisthesis. J Spinal Disord Tech. 2008;21:229–34. - PubMed
-
- Lee CK, Kopacz KJ. In: Rothman “ Simeone the Spine. Herkowitz HN, Garfin SR, Eismont FJ, Bell GR, Balderston RA, editors. Philadelphia: Elsevier; 2006. pp. 350–60.
-
- Cloward RB. The treatment of ruptured lumbar intervertebral discs by vertebral body fusion. I. Indications, operative technique, after care. J Neurosurg. 1953;10:154–68. - PubMed
-
- Brantigan JW, Steffee AD. A carbon fiber implant to aid interbody lumbar fusion. Two-year clinical results in the first 26 patients. Spine (Phila Pa 1976) 1993;18:2106–7. - PubMed
-
- Okuyama K, Kido T, Unoki E, Chiba M. PLIF with a titanium cage and excised facet joint bone for degenerative spondylolisthesis “ In augmentation with a pedicle screw. J Spinal Disord Tech. 2007;20:53–9. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
