

Importance of Frontal Horn Ratio and Optimal CSF Drainage in the Treatment of Very Low-Pressure Hydrocephalus
- PMID: 30009119
- PMCID: PMC6043177
- DOI: 10.1055/s-0037-1609033
Importance of Frontal Horn Ratio and Optimal CSF Drainage in the Treatment of Very Low-Pressure Hydrocephalus
Abstract
Introduction Unlike low-pressure hydrocephalus, very low pressure hydrocephalus (VLPH) is a rarely reported clinical entity previously described to be associated with poor outcomes and to be possibly refractory to treatment with continued cerebrospinal fluid (CSF) drainage at subatmospheric pressures. 1, 2 We present four cases of VLPH following resection of suprasellar lesions and hypothesize that untreatable patients can be identified early, thereby avoiding futile prolonged external ventricular drainage in ICU. Methods We performed a retrospective chart review of four cases of VLPH encountered between 2007 and 2015 in two different institutions and practices and tried to identify factors contributing to successful treatment. We hypothesized that normalization of frontal horn ratio (FHR), optimization of volume of CSF drained, and avoidance of fluid shifts would contribute to improved Glasgow Coma Score (GCS). We examined fluid shifts by studying net fluids shifts and serum levels of sodium, urea, and creatinine. We used Pearson and Spearman correlations to identify measures that would correlate with improved GCS. Results Our study reveals that improving GCS is positively correlated with decreased FHR and increased CSF drainage within an optimal range. The most important determinant of good outcome is retention of brain viscoelasticity as evidenced by restoration and maintenance of good GCS score despite fluctuations in FHR. Conclusion Futile prolonged subatmospheric drainage can be avoided by declining to continue treatment in patients who have permanently altered brain compliance secondary to unsealed CSF leaks, irremediable ventriculitis, and who are therefore unable to sustain an improved neurologic examination.
Keywords: CSF leak; anterior skull base surgery; frontal horn ratio; suprasellar lesions; transsphenoidal surgery; very low pressure hydrocephalus (VLPH).
Figures








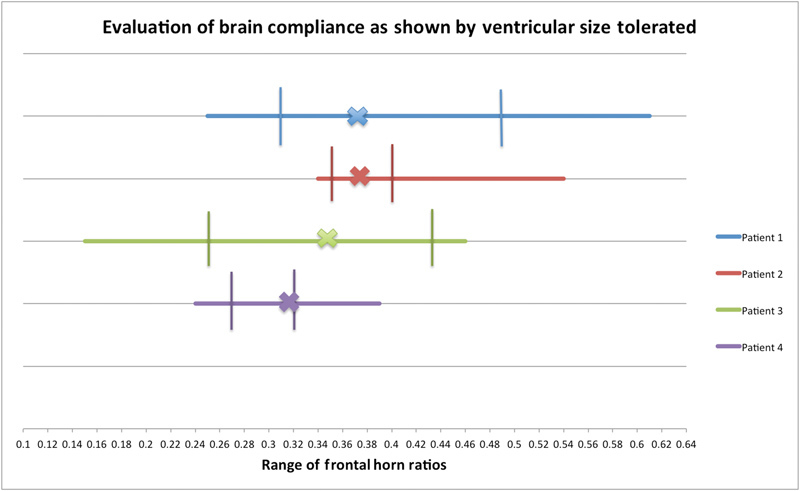
 Response to treatment is not limited by variability in FHR. The vertical lines show the range in which the patients' FHR can vary while maintaining a GCS of 15. The X on each line represents each patients' baseline FHR. Poor compliance predisposes the patient to unsuccessful treatment. Patient 1 had an irreversibly floppy brain. Patient 2 had an abnormally stiff brain. Patient 3 had regained almost normal brain compliance. Patient 4 had regained his baseline brain stiffness. Abbreviations: FHR, frontal horn ratio; GCS, Glasgow Coma Score.
Response to treatment is not limited by variability in FHR. The vertical lines show the range in which the patients' FHR can vary while maintaining a GCS of 15. The X on each line represents each patients' baseline FHR. Poor compliance predisposes the patient to unsuccessful treatment. Patient 1 had an irreversibly floppy brain. Patient 2 had an abnormally stiff brain. Patient 3 had regained almost normal brain compliance. Patient 4 had regained his baseline brain stiffness. Abbreviations: FHR, frontal horn ratio; GCS, Glasgow Coma Score.References
-
- Pang D, Altschuler E.Low-pressure hydrocephalic state and viscoelastic alterations in the brain Neurosurgery 19943504643–655., discussion 655–656 - PubMed
-
- Hamilton M G, Price A V. Syndrome of inappropriately low-pressure acute hydrocephalus (SILPAH) Acta Neurochir Suppl (Wien) 2012;113:155–159. - PubMed
-
- Rekate H L, Nadkarni T D, Wallace D. The importance of the cortical subarachnoid space in understanding hydrocephalus. J Neurosurg Pediatr. 2008;2(01):1–11. - PubMed
-
- Akins P T, Guppy K H, Axelrod Y V, Chakrabarti I, Silverthorn J, Williams A R. The genesis of low pressure hydrocephalus. Neurocrit Care. 2011;15(03):461–468. - PubMed
-
- Clarke M J, Maher C O, Nothdurft G, Meyer F. Very low pressure hydrocephalus. Report of two cases. J Neurosurg. 2006;105(03):475–478. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
