

Accuracy of bone resection in total knee arthroplasty using CT assisted-3D printed patient specific cutting guides
- PMID: 30009760
- PMCID: PMC6047362
- DOI: 10.1051/sicotj/2018032
Accuracy of bone resection in total knee arthroplasty using CT assisted-3D printed patient specific cutting guides
Abstract
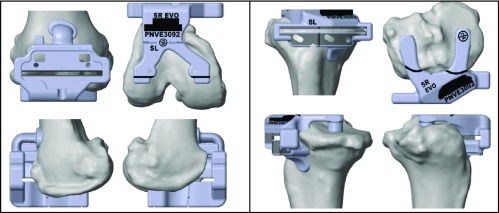
Introduction: We conducted this study to determine if the pre-surgical patient specific instrumented planning based on Computed Tomography (CT) scans can accurately predict each of the femoral and tibial resections performed through 3D printed cutting guides. The technique helps in optimization of component positioning determined by accurate bone resection and hence overall alignment thereby reducing errors.
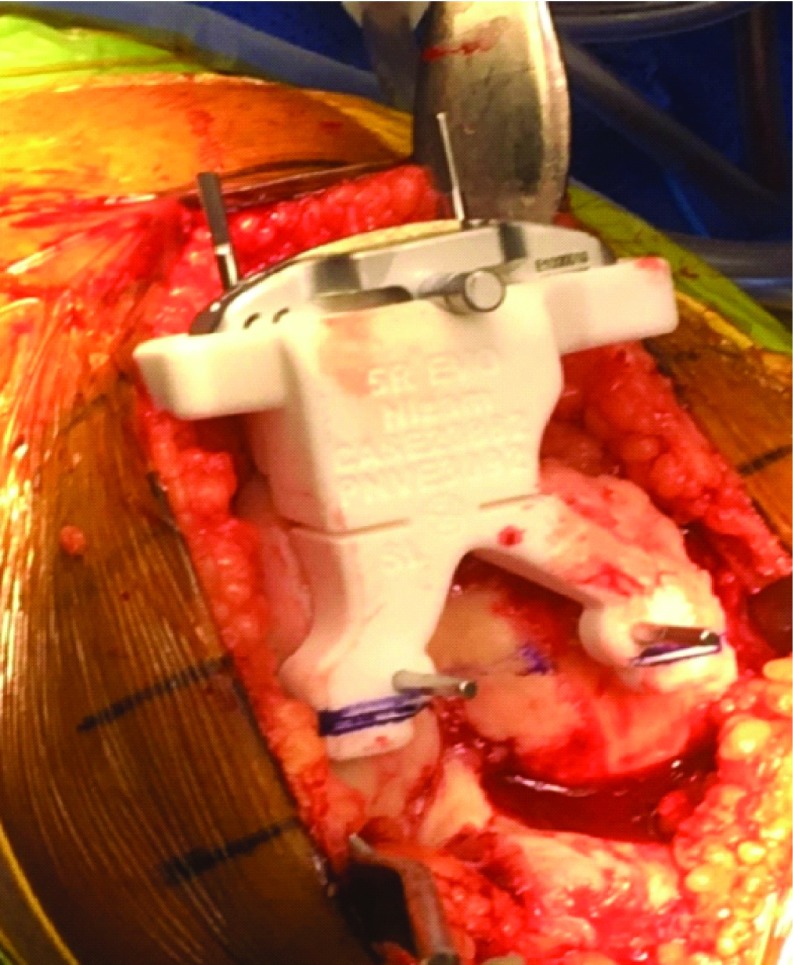
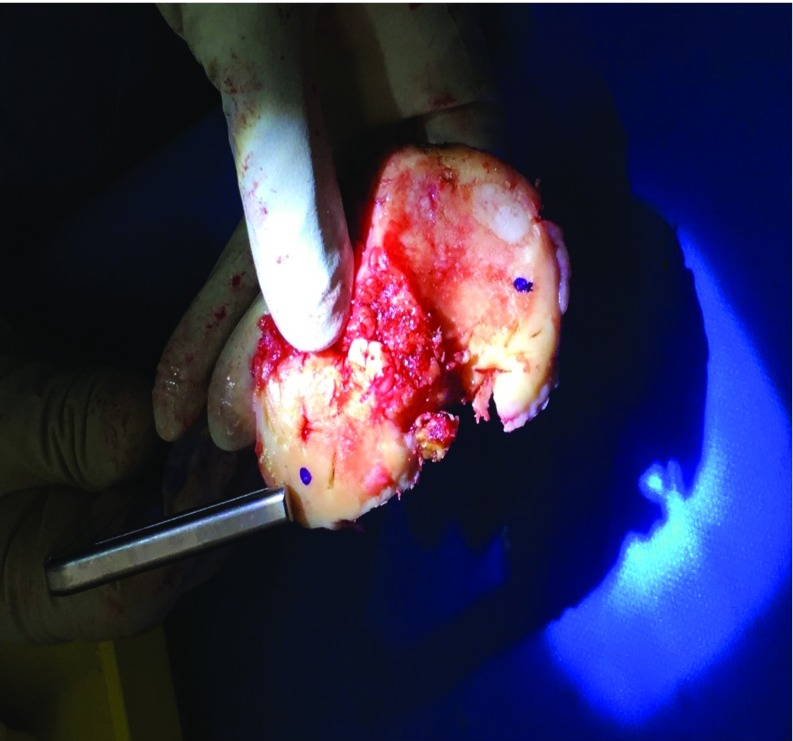
Methods: Prophecy evolution medial pivot patient specific instrumented knee replacement systems were used for end stage arthrosis in all consecutive cases over a period of 20 months by a single surgeon. All resections (4 femoral and 2 tibial) were measured using a vernier callipers intraoperatively. These respective measurements were then compared with the preoperative CT predicted bone resection surgical plan to determine margins of errors that were categorized into 7 groups (0 mm to ≥2.6 mm).
Results: A total of 3618 measurements (averaged to 1206) were performed in 201 knees (105 right and 96 left) in 188 patients (112 females and 76 males) with an average age of 67.72 years (44 to 90 years) and average BMI of 32.3 (25.1 to 42.3). 94% of all collected resection readings were below the error margin of ≤1.5 mm of which 90% showed resection error of ≤1 mm. Mean error of different resections were ≤0.60 mm (P ≤ 0.0001). In 24% of measurements there were no errors or deviations from the templated resection (0.0 mm).
Conclusion: The 3D printed cutting blocks with slots for jigs accurately predict bone resections in patient specific instrumentation total knee arthroplasty which would directly affect component positioning.
© The Authors, published by EDP Sciences, 2018.
Figures


References
-
- Fehring TK, Odum SM, Troyer JL, Iorio R, Kurtz SM, Lau EC (2010) Joint replacement access in 2016: a supply side crisis. J Arthroplast 25(8), 1175–1181. - PubMed
-
- Chareancholvanich K, Narkbunnam R, Pornrattanamaneewong C (2013) A prospective randomisedcontrolled study of patient-specific cutting guides compared with conventional instrumentation in total knee replacement. Bone Joint J 95-B(3), 354–359. - PubMed
-
- Noble JW Jr, Moore CA, Liu N (2012) The value of patient-matched instrumentation in total knee arthroplasty. J Arthroplast 27(1), 153–155. - PubMed
-
- Kim Yh (2001) Incidence of fat embolism syndrome after cemented or cementless bilateral simultaneous and unilateral total knee arthroplasty. J Arthroplast 16(6), 730–739. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources