

Age and Sex Are Critical Factors in Ischemic Stroke Pathology
- PMID: 30010821
- PMCID: PMC6963709
- DOI: 10.1210/en.2018-00465
Age and Sex Are Critical Factors in Ischemic Stroke Pathology
Abstract
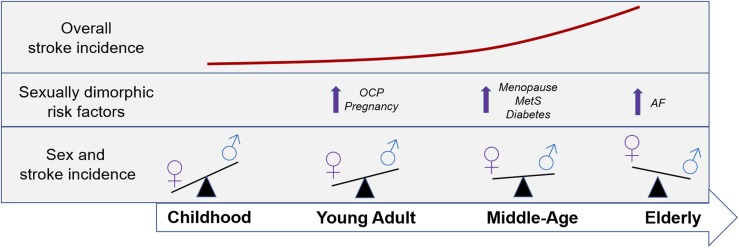
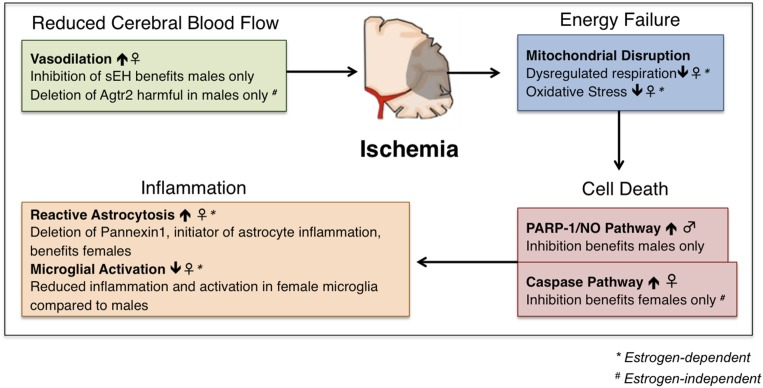
Ischemic stroke is a devastating brain injury resulting in high mortality and substantial loss of function. Understanding the pathophysiology of ischemic stroke risk, mortality, and functional loss is critical to the development of new therapies. Age and sex have a complex and interactive effect on ischemic stroke risk and pathophysiology. Aging is the strongest nonmodifiable risk factor for ischemic stroke, and aged stroke patients have higher mortality and morbidity and poorer functional recovery than their young counterparts. Importantly, patient age modifies the influence of patient sex in ischemic stroke. Early in life, the burden of ischemic stroke is higher in men, but stroke becomes more common and debilitating for women in elderly populations. The profound effects of sex and age on clinical ischemic stroke are mirrored in the results of experimental in vivo and in vitro studies. Here, we review current knowledge on the influence of age and sex in the incidence, mortality, and functional outcome of ischemic stroke in clinical populations. We also discuss the experimental evidence for sex and age differences in stroke pathophysiology and how a better understanding of these biological variables can improve clinical care and enhance development of novel therapies.
Figures
References
-
- Feigin VL, Lawes CM, Bennett DA, Anderson CS. Stroke epidemiology: a review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century. Lancet Neurol. 2003;2(1):43–53. - PubMed
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jiménez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P; American Heart Association Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics-2017 update: a report from the American Heart Association [published correction appears in Circulation. 2017;135(10):e646 and 2017;136(10):e196] Circulation. 2017;135(10):e146–e603. - PMC - PubMed
-
- Arboix A, García-Eroles L, Massons J, Oliveres M, Targa C. Acute stroke in very old people: clinical features and predictors of in-hospital mortality. J Am Geriatr Soc. 2000;48(1):36–41. - PubMed
-
- Dennis MS, Burn JP, Sandercock PA, Bamford JM, Wade DT, Warlow CP. Long-term survival after first-ever stroke: the Oxfordshire Community Stroke Project. Stroke. 1993;24(6):796–800. - PubMed
-
- Di Carlo A, Lamassa M, Pracucci G, Basile AM, Trefoloni G, Vanni P, Wolfe CD, Tilling K, Ebrahim S, Inzitari D; European BIOMED Study of Stroke Care Group . Stroke in the very old : clinical presentation and determinants of 3-month functional outcome: a European perspective. Stroke. 1999;30(11):2313–2319. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
