

Preventing false discovery of heterogeneous treatment effect subgroups in randomized trials
- PMID: 30012181
- PMCID: PMC6048878
- DOI: 10.1186/s13063-018-2774-5
Preventing false discovery of heterogeneous treatment effect subgroups in randomized trials
Abstract
Background: Heterogeneous treatment effects (HTEs), or systematic differences in treatment effectiveness among participants with different observable features, may be important when applying trial results to clinical practice. Current methods suffer from a potential for false detection of HTEs due to imbalances in covariates between candidate subgroups.
Methods: We introduce a new method, matching plus classification and regression trees (mCART), that yields balance in covariates in identified HTE subgroups. We compared mCART to a classical method (logistic regression [LR] with backwards covariate selection using the Akaike information criterion ) and two machine-learning approaches increasingly applied to HTE detection (random forest [RF] and gradient RF) in simulations with a binary outcome with known HTE subgroups. We considered an N = 200 phase II oncology trial where there were either no HTEs (1A) or two HTE subgroups (1B) and an N = 6000 phase III cardiovascular disease trial where there were either no HTEs (2A) or four HTE subgroups (2B). Additionally, we considered an N = 6000 phase III cardiovascular disease trial where there was no average treatment effect but there were four HTE subgroups (2C).
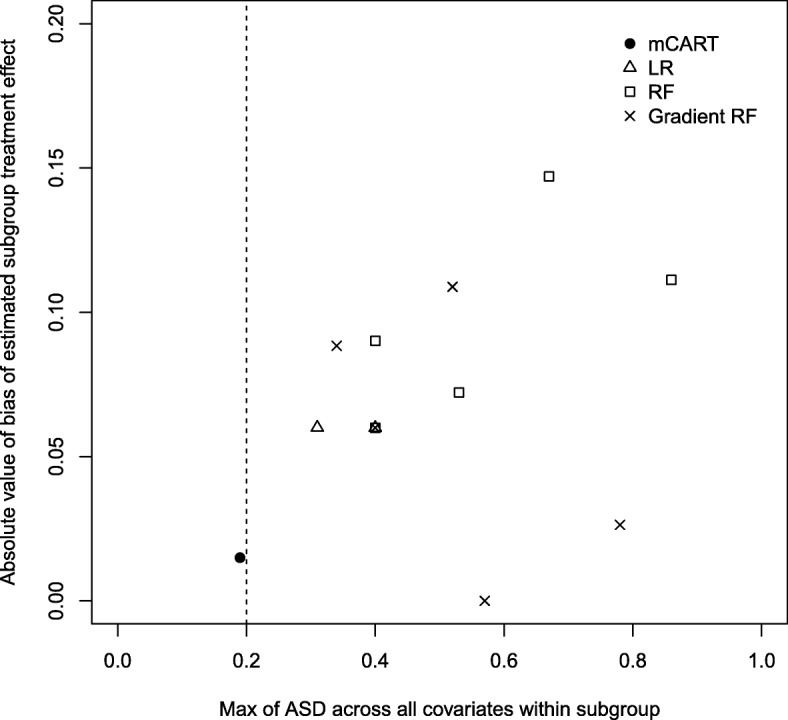
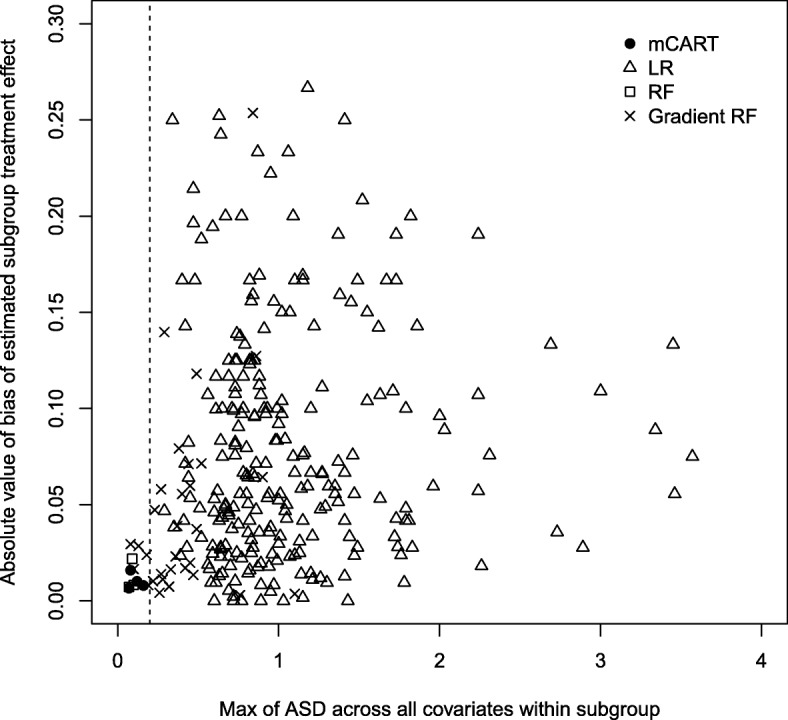
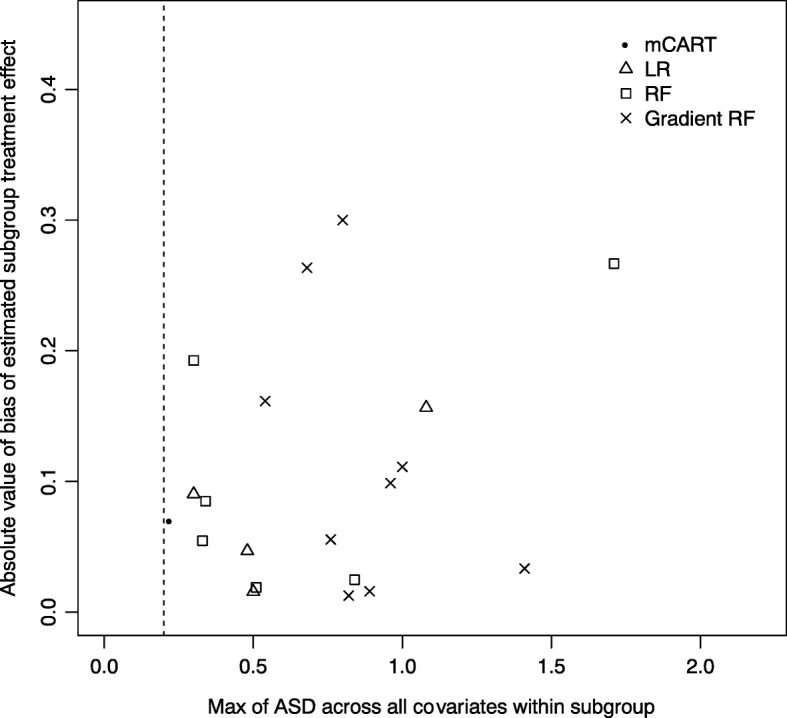
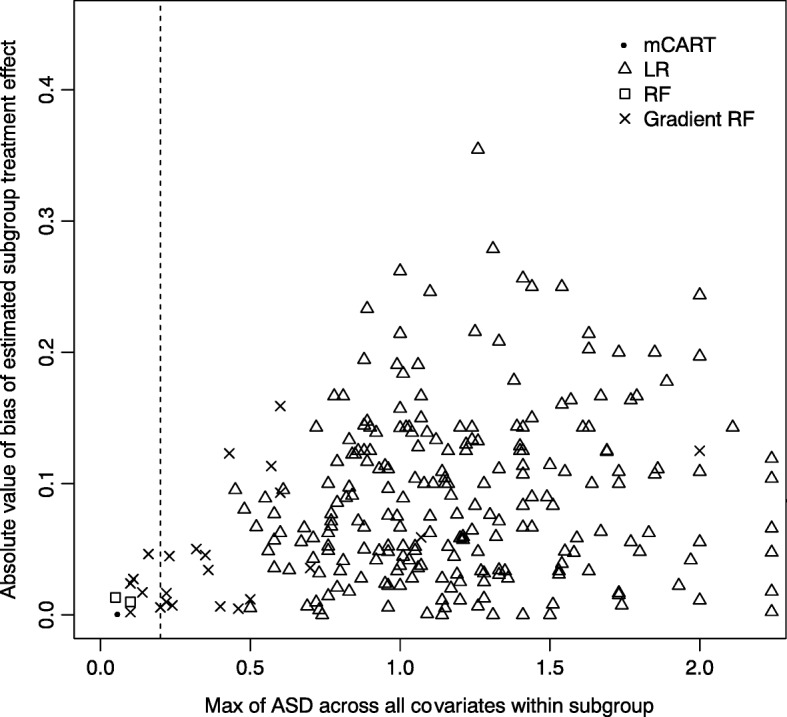
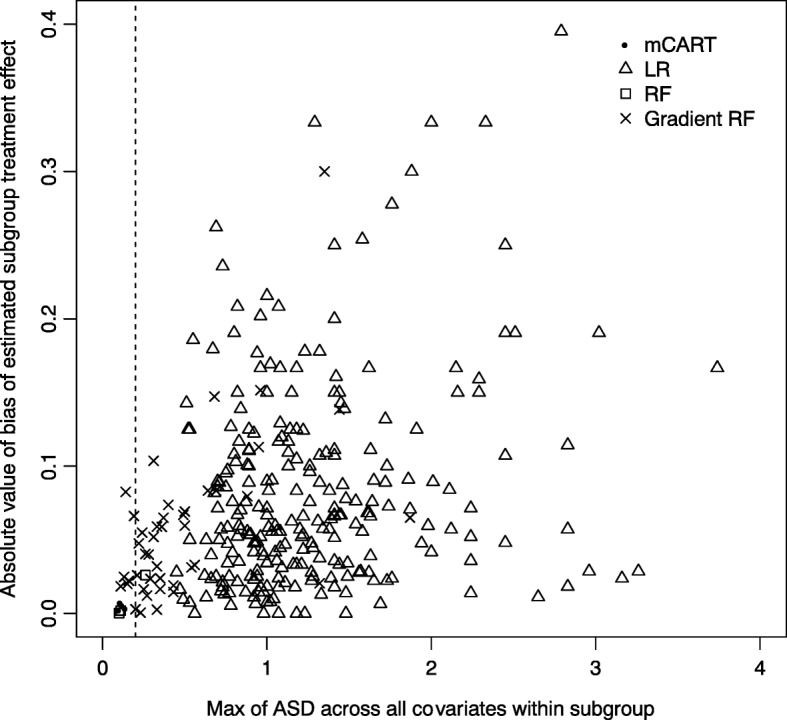
Results: In simulations 1A and 2A (no HTEs), mCART did not identify any HTE subgroups, whereas LR found 2 and 448, RF 5 and 2, and gradient RF 5 and 24, respectively (all false positives). In simulation 1B, mCART failed to identify the two true HTE subgroups whereas LR found 4, RF 6, and gradient RF 10 (half or more of which were false positives). In simulations 2B and 2C, mCART captured the four true HTE subgroups, whereas the other methods found only false positives. All HTE subgroups identified by mCART had acceptable treated vs. control covariate balance with absolute standardized differences less than 0.2, whereas the absolute standardized differences for the other methods typically exceeded 0.2. The imbalance in covariates in identified subgroups for LR, RF, and gradient RF indicates the false HTE detection may have been due to confounding.
Conclusions: Covariate imbalances may be producing false positives in subgroup analyses. mCART could be a useful tool to help prevent the false discovery of HTE subgroups in secondary analyses of randomized trial data.
Keywords: Classification and regression trees; Decision support tool; Heterogeneous treatment effects; Matching.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Baum A, Scarpa J, Bruzelius E, Tamler R, Basu S, Faghmous J. Targeting weight loss interventions to reduce cardiovascular complications of type 2 diabetes: a machine learning-based post-hoc analysis of heterogeneous treatment effects in the look AHEAD trial. Lancet Diabetes Endocrinol. 2017;5:808–815. doi: 10.1016/S2213-8587(17)30176-6. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
