

The Society for Immunotherapy of Cancer consensus statement on immunotherapy for the treatment of non-small cell lung cancer (NSCLC)
- PMID: 30012210
- PMCID: PMC6048854
- DOI: 10.1186/s40425-018-0382-2
The Society for Immunotherapy of Cancer consensus statement on immunotherapy for the treatment of non-small cell lung cancer (NSCLC)
Abstract
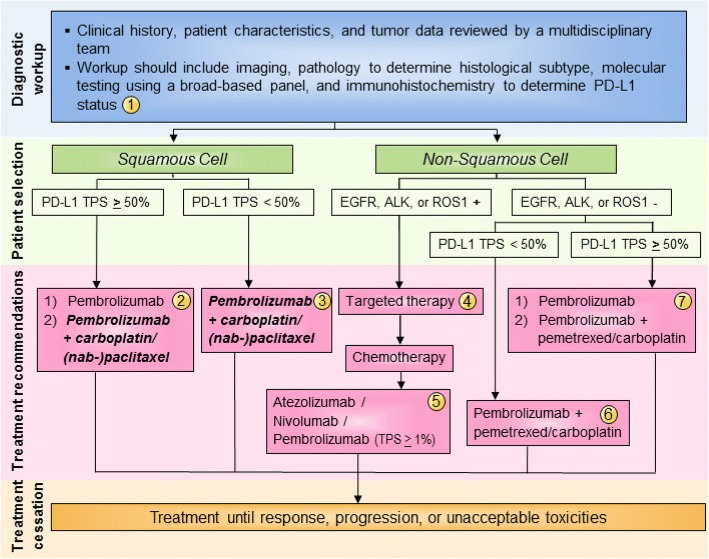
Lung cancer is the leading cause of cancer-related mortality worldwide, with non-small cell lung cancer (NSCLC) accounting for over 85% of all cases. Until recently, chemotherapy - characterized by some benefit but only rare durable responses - was the only treatment option for patients with NSCLC whose tumors lacked targetable mutations. By contrast, immune checkpoint inhibitors have demonstrated distinctly durable responses and represent the advent of a new treatment approach for patients with NSCLC. Three immune checkpoint inhibitors, pembrolizumab, nivolumab and atezolizumab, are now approved for use in first- and/or second-line settings for selected patients with advanced NSCLC, with promising benefit also seen in patients with stage III NSCLC. Additionally, durvalumab following chemoradiation has been approved for use in patients with locally advanced disease. Due to the distinct features of cancer immunotherapy, and rapid progress in the field, clinical guidance is needed on the use of these agents, including appropriate patient selection, sequencing of therapies, response monitoring, adverse event management, and biomarker testing. The Society for Immunotherapy of Cancer (SITC) convened an expert Task Force charged with developing consensus recommendations on these key issues. Following a systematic process as outlined by the National Academy of Medicine, a literature search and panel voting were used to rate the strength of evidence for each recommendation. This consensus statement provides evidence-based recommendations to help clinicians integrate immune checkpoint inhibitors into the treatment plan for patients with NSCLC. This guidance will be updated following relevant advances in the field.
Keywords: Cancer immunotherapy; Consensus statement; Guideline; Lung cancer; Non-small cell lung cancer.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
JRB has participated on advisory boards and/or served as a consultant to Bristol-Myers Squibb, Merck, Celgene, and Eli Lilly. In addition, she has received research funding/grant support from Bristol-Myers Squibb, MedImmune/AstraZeneca, and Merck. RG has received honoraria for his service on the advisory board at Abbvie and for consulting with Genentech/Roche. He has also served on the advisory boards of Inivata, Pfizer, EMD Serono, AstraZeneca, and Bristol-Myers Squibb. RAA has received financial research support from from Bristol-Myers Squibb, Merck Sharpe & Dohme, Five Prime Therapeutics, Stand Up 2 Cancer, the National Institutes of Health and FLX Bio. SJA participates on the advisory boards for Bristol-Myers Squibb, Novartis, Merck, Cellular Biomedicine Group, Boehringer Ingelheim, AstraZeneca/MedImmune, Memgen, and FLX Bio. He also has a research contract with Novartis. SS has received an honorarium from Bristol-Myers Squibb. MJD has participated in speakers bureaus for Bristol-Myers Squibb, AstraZeneca, Genentech/Roche and Merck. SMD serves on the advisory board at AstraZeneca. LG serves on the advisory boards at Genentech/Roche, Merck, AstraZeneca, Ignyta and Syndax. Additionally, she receives institutional research support from Bristol-Myers Squibb. EBG has received institutional research support from AstraZeneca, Merck, Bristol-Myers Squibb, Boehringer Ingelheim, Genentech/Roche, Eli Lilly, Pfizer, Mirati, Dynavax and Novartis. MDH has received financial support for the provision of consultation services to Genentech/Roche, Merck, Bristol-Myers Squibb, AstraZeneca, Mirati, Janssen, and Shattuck Labs. Additionally, MDH has received research funding from Bristol-Myers Squibb. FRH serves on scientific advisory boards for Bristol-Myers Squibb, Genentech/Roche, Merck, AstraZeneca, Ventana, HTG Molecular Diagnostics, Biocept, Eli Lilly, Loxo Oncology, Abbvie, Novartis and Pfizer. JWN serves as an advisor and/or provides consultation to Clovis Oncology, Boehringer Ingelheim, Takeda, and Eli Lilly. In addition, he has received institutional research support from Genentech/Roche, Merck, Novartis, Exelixis, Boehringer Ingelheim, and Nektar. VAP has been a steering committee member on the advisory boards at Merck, AstraZeneca, Bristol-Myers Squibb, Nektar Therapeutics and Genentech/Roche. DLR is a consultant and advisor for Bristol-Myers Squibb, Merck, A2 Pharma, and Cell Signaling Technology. Additionally, his lab receives research support from AstraZeneca and Eli Lilly. LHS has provided consultation and endpoint analysis, and is a member of the Data Safety and Monitoring Boards for Merck and Novartis. BYY’s spouse serves on the scientific advisory board at the LUNGevity Foundation. NAR is a co-founder and shareholder of Gritstone Oncology, is on the Board of Directors for and is a shareholder of ARMO Bioscience, and has served on the advisory boards at Bristol-Myers Squibb, Genentech/Roche, AstraZeneca, Merck, EMD Serono, Pfizer, Eli Lilly, Abbvie, Regeneron, and Novartis. RSH has served as a consultant to AstraZeneca, Eli Lilly, Genentech/Roche, Merck, and Pfizer. In addition, he has received clinical trial support/grants from Genentech/Roche and Merck. AF, SM, and BS declare no competing interests.
Figures
References
-
- About non-small cell lung cancer [https://www.cancer.org/content/dam/CRC/PDF/Public/8703.00.pdf].
-
- SEER stat fact sheets: lung and bronchus cancer [http://seer.cancer.gov/statfacts/html/lungb.html].
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases