

Early detection and treatment strategies for breast cancer in low-income and upper middle-income countries: a modelling study
- PMID: 30012269
- PMCID: PMC6214657
- DOI: 10.1016/S2214-109X(18)30257-2
Early detection and treatment strategies for breast cancer in low-income and upper middle-income countries: a modelling study
Abstract
Background: Poor breast cancer survival in low-income and middle-income countries (LMICs) can be attributed to advanced-stage presentation and poor access to systemic therapy. We aimed to estimate the outcomes of different early detection strategies in combination with systemic chemotherapy and endocrine therapy in LMICs.
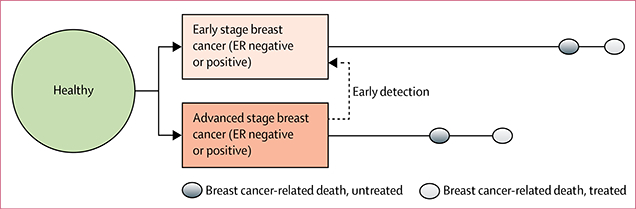
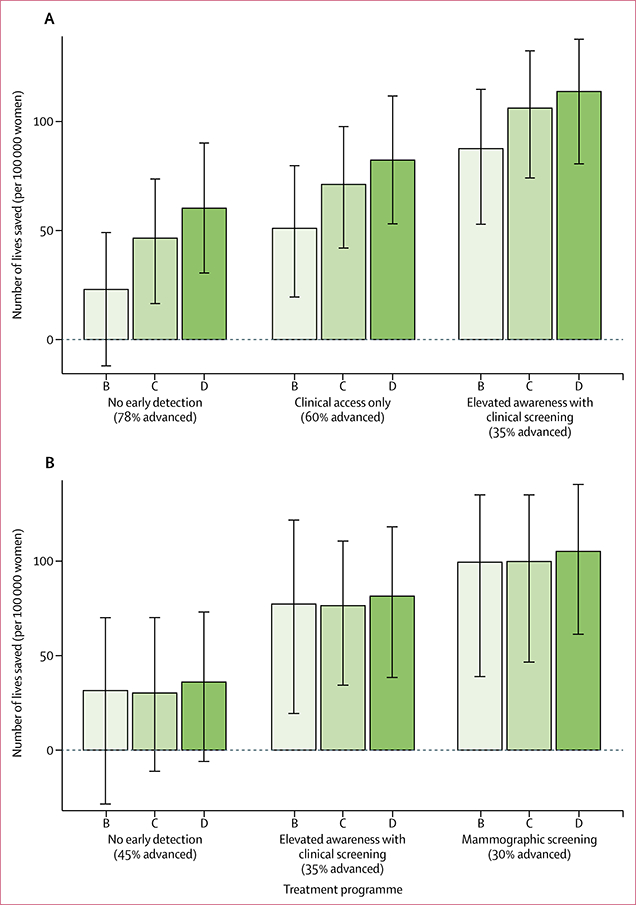
Methods: We adapted a microsimulation model to project outcomes of three early detection strategies alone or in combination with three systemic treatment programmes beyond standard of care (programme A): programme B was endocrine therapy for all oestrogen-receptor (ER)-positive cases; programme C was programme B plus chemotherapy for ER-negative cases; programme D was programme C plus chemotherapy for advanced ER-positive cases. The main outcomes were reductions in breast cancer-related mortality and lives saved per 100 000 women relative to the standard of care for women aged 30-49 years in a low-income setting (East Africa; using incidence data and life tables from Uganda and data on tumour characteristics from various East African countries) and for women aged 50-69 years in a middle-income setting (Colombia).
Findings: In the East African setting, relative mortality reductions were 8-41%, corresponding to 23 (95% uncertainty interval -12 to 49) to 114 (80 to 138) lives saved per 100 000 women over 10 years. In Colombia, mortality reductions were 7-25%, corresponding to 32 (-29 to 70) to 105 (61 to 141) lives saved per 100 000 women over 10 years.
Interpretation: The best projected outcomes were in settings where access to both early detection and adjuvant therapy is improved. Even in the absence of mammographic screening, improvements in detection can provide substantial benefit in settings where advanced-stage presentation is common.
Funding: Fred Hutchinson Cancer Research Center/University of Washington Cancer Consortium Cancer Center Support Grant of the US National Institutes of Health.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an open access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests
We declare no competing interests.
Figures
Comment in
-
All simulation models of breast cancer are wrong but some are useful.Lancet Glob Health. 2018 Aug;6(8):e818-e819. doi: 10.1016/S2214-109X(18)30273-0. Lancet Glob Health. 2018. PMID: 30012255 No abstract available.
References
-
- DeSantis CE, Lin CC, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2014. CA Cancer J Clin 2014; 64: 252–71. - PubMed
-
- Berry DA, Cronin KA, Plevritis SK, et al. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med 2005; 353: 1784–92. - PubMed
-
- Coleman MP, Quaresma M, Berrino F, et al. Cancer survival in five continents: a worldwide population-based study (CONCORD). Lancet Oncol 2008; 9: 730–56. - PubMed
-
- Anderson BO, Yip CH, Smith RA, et al. Guideline implementation for breast healthcare in low-income and middle-income countries: overview of the Breast Health Global Initiative Global Summit 2007. Cancer 2008; 113: 2221–3. - PubMed
-
- Shyyan R, Sener SF, Anderson BO, et al. Guideline implementation for breast healthcare in low- and middle-income countries: diagnosis resource allocation. Cancer 2008; 113: 2257–68. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
