

Incretin-Based Therapies and Diabetic Retinopathy: Real-World Evidence in Older U.S. Adults
- PMID: 30012674
- PMCID: PMC6105327
- DOI: 10.2337/dc17-2285
Incretin-Based Therapies and Diabetic Retinopathy: Real-World Evidence in Older U.S. Adults
Abstract
Objective: Recent large trials yield conflicting results on the association between incretin-based therapies (IBTs) and diabetic retinopathy (DR). We examined whether IBTs increase DR risk compared with other antihyperglycemics.
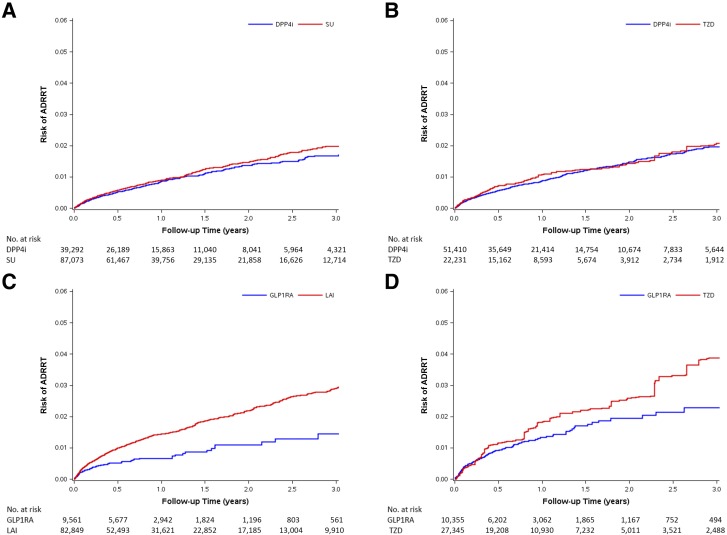
Research design and methods: We implemented an active comparator, new-user cohort design using a nationwide 20% random sample of fee-for-service U.S. Medicare beneficiaries aged 65 years or older with Parts A, B, and D coverage between 2007 and 2015. We identified the following cohorts without prior treatment for retinopathy: dipeptidyl peptidase 4 inhibitors (DPP4i) versus sulfonylureas (SU), DPP4i versus thiazolidinediones (TZD), glucagon-like peptide-1 receptor agonists (GLP1RA) versus long-acting insulin (LAI), and GLP1RA versus TZD. Primary outcome was advanced diabetic retinopathy requiring treatment (ADRRT), defined as a procedure code for retinopathy treatment. Incident diabetic retinopathy (IDR), identified by a diagnosis code, was a secondary outcome. We estimated propensity scores to balance confounders and adjusted hazard ratios (95% CI) using weighted Cox proportional hazards models.
Results: We identified 213,652 eligible patients. During a median duration of 0.58 to 0.87 years across comparisons, with a rate from 6.0 to 12.8 per 1,000 person-years, IBTs were not associated with increased ADRRT or IDR risk. The adjusted hazard ratios (95% CI) for ADRRT were 0.91 (0.79-1.04) by comparing DPP4i to SU (n = 39,292 and 87,073); 0.91 (0.75-1.11), DPP4i to TZD (n = 51,410 and 22,231); 0.50 (0.39-0.65), GLP1RA to LAI (n = 9,561 and 82,849); and 0.75 (0.53-1.06), GLP1RA to TZD (n = 10,355 and 27,345).
Conclusions: Our population-based cohort study of older U.S. adults with diabetes suggests that IBTs used for approximately 1 year do not increase the DR risk.
© 2018 by the American Diabetes Association.
Figures
Comment in
-
Comment on Wang et al. Incretin-Based Therapies and Diabetic Retinopathy: Real-World Evidence in Older U.S. Adults. Diabetes Care 2018;41:1998-2009.Diabetes Care. 2019 Jan;42(1):e8. doi: 10.2337/dc18-1825. Diabetes Care. 2019. PMID: 30811336 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL118255/HL/NHLBI NIH HHS/United States
- U10 EY018817/EY/NEI NIH HHS/United States
- R01 AG023178/AG/NIA NIH HHS/United States
- R21 HD080214/HD/NICHD NIH HHS/United States
- R56 AG023178/AG/NIA NIH HHS/United States
- R01 AG056479/AG/NIA NIH HHS/United States
- UL1 TR001111/TR/NCATS NIH HHS/United States
- UG1 EY014231/EY/NEI NIH HHS/United States
- U10 EY014231/EY/NEI NIH HHS/United States
- U10 EY014269/EY/NEI NIH HHS/United States
- UL1 TR002489/TR/NCATS NIH HHS/United States
- U10 EY014229/EY/NEI NIH HHS/United States
- R01 CA174453/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
