

Phantom motor execution as a treatment for phantom limb pain: protocol of an international, double-blind, randomised controlled clinical trial
- PMID: 30012784
- PMCID: PMC6082487
- DOI: 10.1136/bmjopen-2017-021039
Phantom motor execution as a treatment for phantom limb pain: protocol of an international, double-blind, randomised controlled clinical trial
Abstract
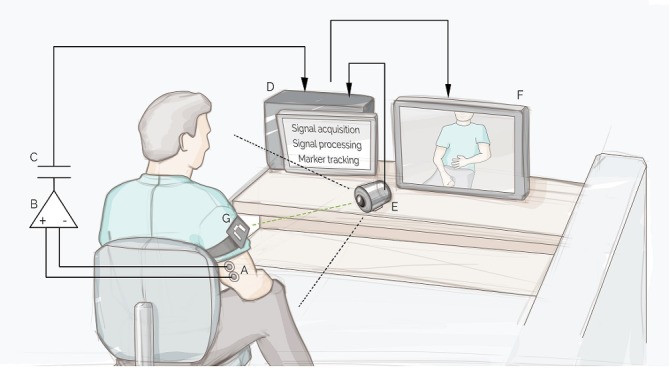
Introduction: Phantom limb pain (PLP) is a chronic condition that can greatly diminish quality of life. Control over the phantom limb and exercise of such control have been hypothesised to reverse maladaptive brain changes correlated to PLP. Preliminary investigations have shown that decoding motor volition using myoelectric pattern recognition, while providing real-time feedback via virtual and augmented reality (VR-AR), facilitates phantom motor execution (PME) and reduces PLP. Here we present the study protocol for an international (seven countries), multicentre (nine clinics), double-blind, randomised controlled clinical trial to assess the effectiveness of PME in alleviating PLP.
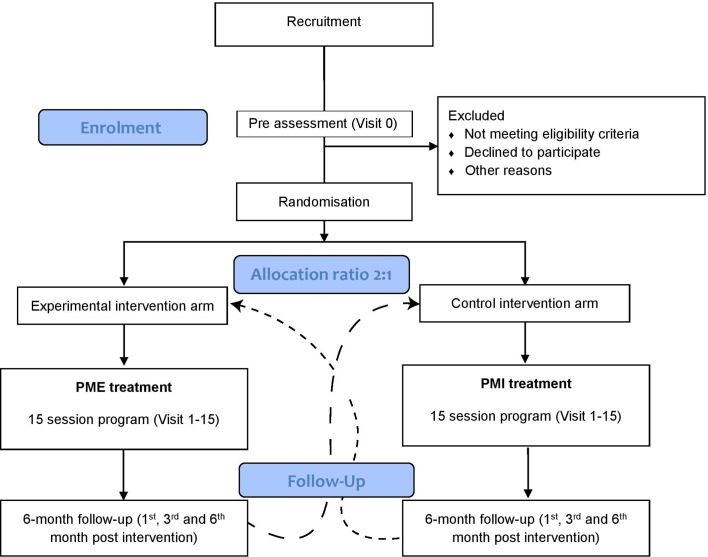
Methods and analysis: Sixty-seven subjects suffering from PLP in upper or lower limbs are randomly assigned to PME or phantom motor imagery (PMI) interventions. Subjects allocated to either treatment receive 15 interventions and are exposed to the same VR-AR environments using the same device. The only difference between interventions is whether phantom movements are actually performed (PME) or just imagined (PMI). Complete evaluations are conducted at baseline and at intervention completion, as well as 1, 3 and 6 months later using an intention-to-treat (ITT) approach. Changes in PLP measured using the Pain Rating Index between the first and last session are the primary measure of efficacy. Secondary outcomes include: frequency, duration, quality of pain, intrusion of pain in activities of daily living and sleep, disability associated to pain, pain self-efficacy, frequency of depressed mood, presence of catastrophising thinking, health-related quality of life and clinically significant change as patient's own impression. Follow-up interviews are conducted up to 6 months after the treatment.
Ethics and dissemination: The study is performed in agreement with the Declaration of Helsinki and under approval by the governing ethical committees of each participating clinic. The results will be published according to the Consolidated Standards of Reporting Trials guidelines in a peer-reviewed journal.
Trial registration number: NCT03112928; Pre-results.
Keywords: clinical trials; neurological pain; rehabilitation medicine.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: The sponsor of this study (Integrum AB) is a for-profit organisation that might commercialise the device used in this study (phantom motor execution and phantom motor imagery). MO-C was partially funded by Integrum AB. The core technology used in this study has been made freely available as open source by MO-C (machine learning, virtual reality and electronics).
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials