

Hypertension, Microvascular Pathology, and Prognosis After an Acute Myocardial Infarction
- PMID: 30012869
- PMCID: PMC6080885
- DOI: 10.1161/HYPERTENSIONAHA.117.10786
Hypertension, Microvascular Pathology, and Prognosis After an Acute Myocardial Infarction
Abstract
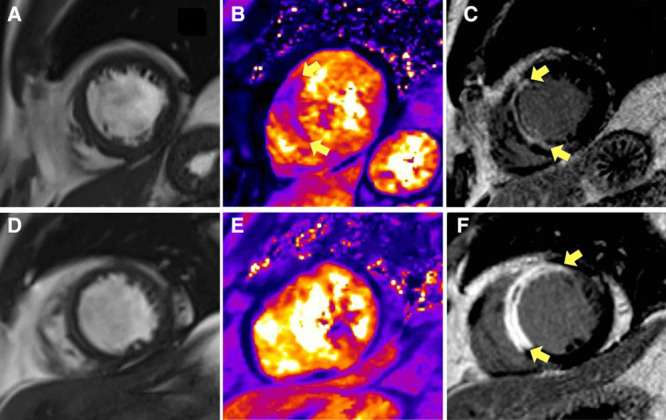
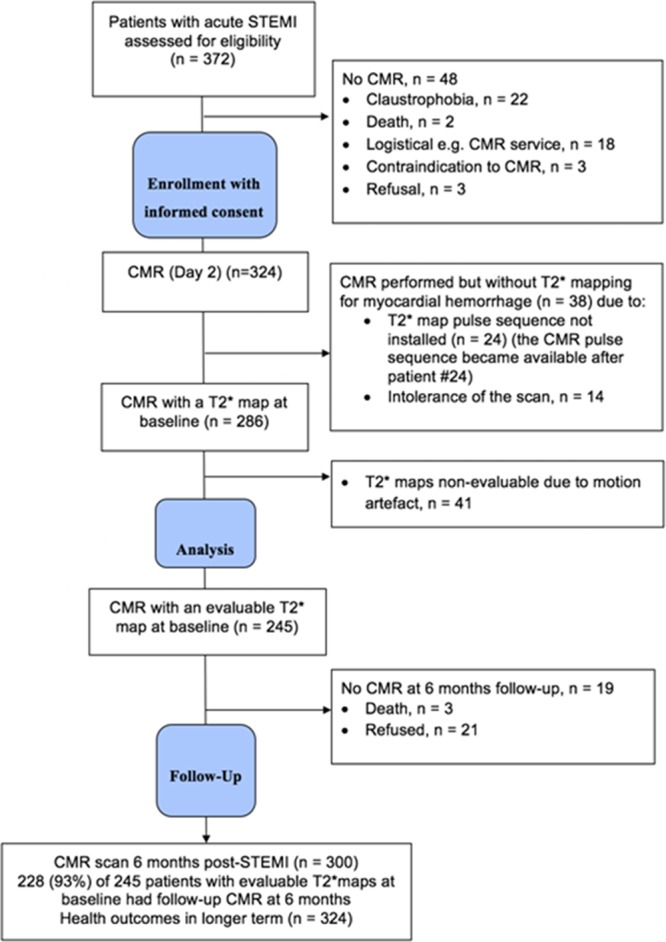
The rationale for our study was to investigate the pathophysiology of microvascular injury in patients with acute ST-segment-elevation myocardial infarction in relation to a history of hypertension. We undertook a cohort study using invasive and noninvasive measures of microvascular injury, cardiac magnetic resonance imaging at 2 days and 6 months, and assessed health outcomes in the longer term. Three hundred twenty-four patients with acute myocardial infarction (mean age, 59 [12] years; blood pressure, 135 [25] / 79 [14] mm Hg; 237 [73%] male, 105 [32%] with antecedent hypertension) were prospectively enrolled during emergency percutaneous coronary intervention. Compared with patients without antecedent hypertension, patients with hypertension were older (63 [12] years versus 57 [11] years; P<0.001) and a lower proportion were cigarette smokers (52 [50%] versus 144 [66%]; P=0.007). Coronary blood flow, microvascular resistance within the culprit artery, infarct pathologies, inflammation (C-reactive protein and interleukin-6) were not associated with hypertension. Compared with patients without antecedent hypertension, patients with hypertension had less improvement in left ventricular ejection fraction at 6 months from baseline (5.3 [8.2]% versus 7.4 [7.6]%; P=0.040). Antecedent hypertension was a multivariable associate of incident myocardial hemorrhage 2-day post-MI (1.81 [0.98-3.34]; P=0.059) and all-cause death or heart failure (n=47 events, n=24 with hypertension; 2.53 [1.28-4.98]; P=0.007) postdischarge (median follow-up 4 years). Severe progressive microvascular injury is implicated in the pathophysiology and prognosis of patients with a history of hypertension and acute myocardial infarction. Clinical Trial Registration- URL: http://www.clinicaltrials.gov . Unique identifier: NCT02072850.
Keywords: atherosclerosis; hypertension; myocardial infarction; prognosis; reperfusion injury.
Figures
References
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–1913. doi: 10.1016/S0140-6736(02)11911-8. - PubMed
-
- Benjamin EJ, Blaha MJ, Chiuve SE, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2017 update: a report from the American Heart Association. Circulation. 2017;135:e146–e603. doi: 10.1161/CIR.0000000000000485. - PMC - PubMed
-
- British Heart Foundation. Cardiovascular Disease Statistics Factsheet (UK). https://www.bhf.org.uk/statistics. Accessed April 27, 2018.
-
- Thune JJ, Signorovitch J, Kober L, Velazquez EJ, McMurray JJ, Califf RM, Maggioni AP, Rouleau JL, Howlett J, Zelenkofske S, Pfeffer MA, Solomon SD. Effect of antecedent hypertension and follow-up blood pressure on outcomes after high-risk myocardial infarction. Hypertension. 2008;51:48–54. doi: 10.1161/HYPERTENSIONAHA.107.093682. - PubMed
-
- Fresco C, Avanzini F, Bosi S, Franzosi MG, Maggioni AP, Santoro L, Bellanti G. Prognostic value of a history of hypertension in 11,483 patients with acute myocardial infarction treated with thrombolysis. GISSI-2 Investigators. Gruppo Italiano per lo Studio della, Sopravvivena nell’Infarto Miocardico. J Hypertens. 1996;14:743–750. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
