

Outcome and prognostic factors in 593 non-metastatic rectal cancer patients: a mono-institutional survey
- PMID: 30013090
- PMCID: PMC6048026
- DOI: 10.1038/s41598-018-29040-2
Outcome and prognostic factors in 593 non-metastatic rectal cancer patients: a mono-institutional survey
Abstract
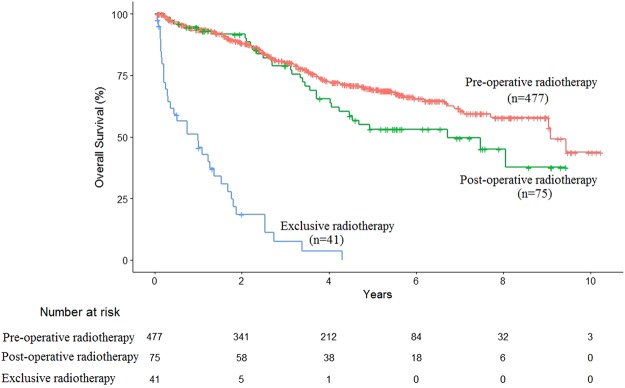
This retrospective study was undertaken to provide more modern data of real-life management of non-metastatic rectal cancer, to compare therapeutic strategies, and to identify prognostic factors of overall survival (OS) in a large cohort of patients. Data on efficacy and on acute/late toxicity were retrospectively collected. Patients were diagnosed a non-metastatic rectal cancer between 2004 and 2015, and were treated at least with radiotherapy. OS was correlated with patient, tumor and treatment characteristics with univariate and multivariate analyses. Data of 593 consecutive non-metastatic rectal cancer patients were analyzed. Median follow-up was 41 months. Median OS was 9 years. Radiotherapy was delivered in pre-operative (n = 477, 80.5%), post-operative (n = 75, 12.6%) or exclusive (n = 41, 6.9%) setting. In the whole set of patients, age, nutritional condition, tumor stage, tumor differentiation, and surgery independently influenced OS. For patients experiencing surgery, OS was influenced by age, tumor differentiation and nodal status. Surgical resection is the cornerstone treatment for locally-advanced rectal cancer. Poor tumor differentiation and node involvement were identified as major predictive factor of poor OS. The research in treatment intensification and in identification of radioresistance biomarkers should therefore probably be focused on this particular subset of patients.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Sauer R, et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012;30:1926–1933. doi: 10.1200/JCO.2011.40.1836. - DOI - PubMed
-
- Kapiteijn E, et al. Local recurrence in patients with rectal cancer diagnosed between 1988 and 1992: a population-based study in the west Netherlands. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 1998;24:528–535. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
