

Transaminase and Creatine Kinase Ratios for Differentiating Delayed Acetaminophen Overdose from Rhabdomyolysis
- PMID: 30013711
- PMCID: PMC6040894
- DOI: 10.5811/westjem.2018.3.37076
Transaminase and Creatine Kinase Ratios for Differentiating Delayed Acetaminophen Overdose from Rhabdomyolysis
Abstract
Introduction: Rhabdomyolysis and delayed acetaminophen hepatotoxicity may be associated with elevated serum transaminase values. Establishing the cause of elevated transaminases may be especially difficult because of limited or inaccurate histories of acetaminophen ingestion. We hypothesized that the comparative ratios of aspartate aminotransferase (AST), alanine aminotransferase (ALT), and creatine kinase (CK) can differentiate acetaminophen hepatotoxicity from rhabdomyolysis.
Methods: A retrospective chart review of patients in four hospitals from 2006 to 2011 with a discharge diagnosis of acetaminophen toxicity or rhabdomyolysis was performed. Subjects were classified into three groups: rhabdomyolysis, acetaminophen overdose (all), and acetaminophen overdose with undetectable serum acetaminophen concentrations [acetaminophen(delayed)]. Ratios of AST, ALT, and CK were compared using non-parametric statistical methods.
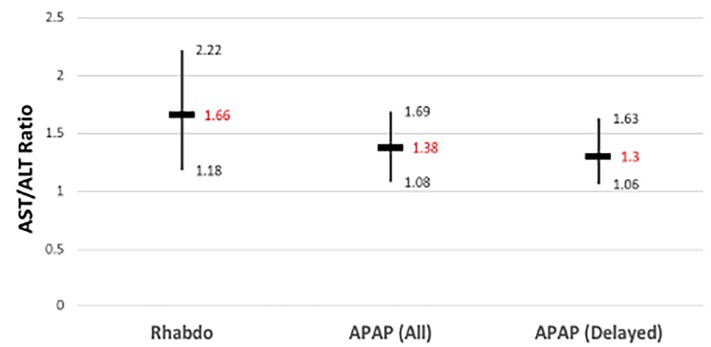
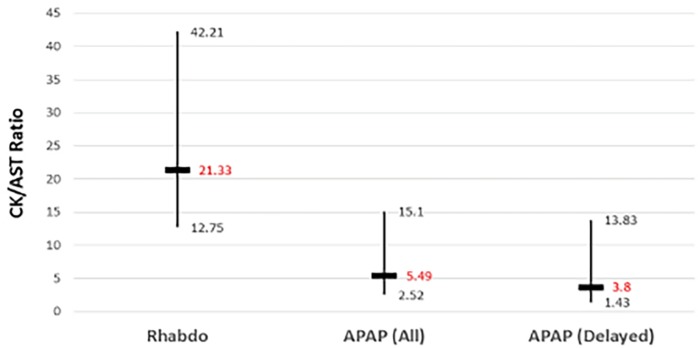
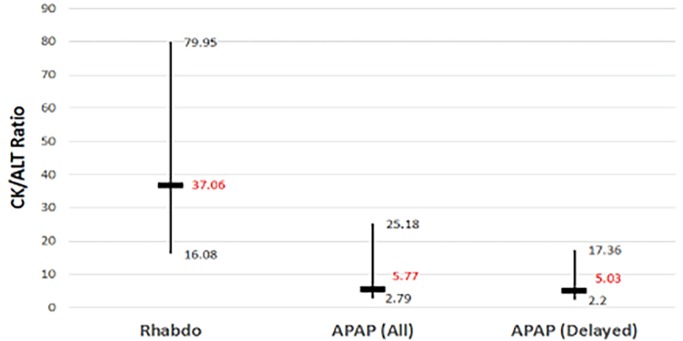
Results: 1,353 subjects were identified and after applying our exclusion criteria there were 160 in the rhabdomyolysis group, 68 in the acetaminophen overdose (all) group, and 29 in the acetaminophen (delayed) group. The AST/ALT ratio for the rhabdomyolysis group was 1.66 (Interquartile range: 1.18-2.22), for the acetaminophen overdose (all) group was 1.38 (1.08-1.69, statistically lower than the rhabdomyolysis group, p = 0.018), and for the acetaminophen (delayed)group was 1.30 (1.06-1.63, p = 0.037). CK/AST ratios were 21.3 (12.8-42.2), 5.49 (2.52-15.1, p < 0.001), and 3.80 (1.43-13.8, p < 0.001) respectively. CK/ALT ratios were 37.1 (16.1-80.0), 5.77 (2.79-25.2, p < 0.001), and 5.03 (2.20-17.4, p < 0.001) respectively. Increasing CK to transaminase ratio cutoffs resulted in increasing test sensitivity but lower specificity.
Conclusion: AST/ALT, CK/AST and CK/ALT ratios are significantly larger in rhabdomyolysis when compared to patients with acetaminophen toxicity. This result suggests that the ratios could be used to identify patients with rhabdomyolysis who otherwise might have been diagnosed as delayed acetaminophen toxicity. Such patients may not require treatment with N-acetylcysteine, resulting in cost savings and improved resource utilization.
Conflict of interest statement
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
Figures
References
-
- Whitfield J. Gamma glutamyl transferase. Crit Rev Clin Lab Sci. 2001;38(4):263–355. - PubMed
-
- Pertusi R, Dickerman R, McConathy W. Evaluation of aminotransferase elevations in a bodybuilder using anabolic steroids: hepatitis or rhabdomyolysis. J Am Osteopath Assoc. 2001;101(7):391–4. - PubMed
-
- Miyazaki M, Resonblum JS, Kasahara Y, et al. Determination of enzymatic source of alanine aminotransferase activity in serum from dogs with liver injury. J Pharmacol Toxicol Methods. 2009;60(3):307–15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials