

doi: 10.1016/j.eats.2018.02.006.
eCollection 2018 Jun.
How to Rapidly Abolish Knee Extension Deficit After Injury or Surgery: A Practice-Changing Video Pearl From the Scientific Anterior Cruciate Ligament Network International (SANTI) Study Group
Affiliations
- PMID: 30013901
- PMCID: PMC6019855
- DOI: 10.1016/j.eats.2018.02.006
Item in Clipboard
How to Rapidly Abolish Knee Extension Deficit After Injury or Surgery: A Practice-Changing Video Pearl From the Scientific Anterior Cruciate Ligament Network International (SANTI) Study Group
Arthrosc Tech.
.
Abstract
Knee extension deficit is frequently observed after anterior cruciate ligament reconstruction or rupture and other acute knee injuries. Loss of terminal extension often occurs because of hamstring contracture and quadriceps inactivation rather than mechanical intra-articular pathology. Failure to regain full extension in the first few weeks after anterior cruciate ligament reconstruction is a recognized risk factor for adverse long-term outcomes, and therefore, it is important to try to address it. In this Technical Note, a simple, rapid, and effective technique to help regain full knee extension and abolish quadriceps activation failure is described.
Figures

Knee extension deficit evaluation of right knee (asterisk) with patient in supine position.
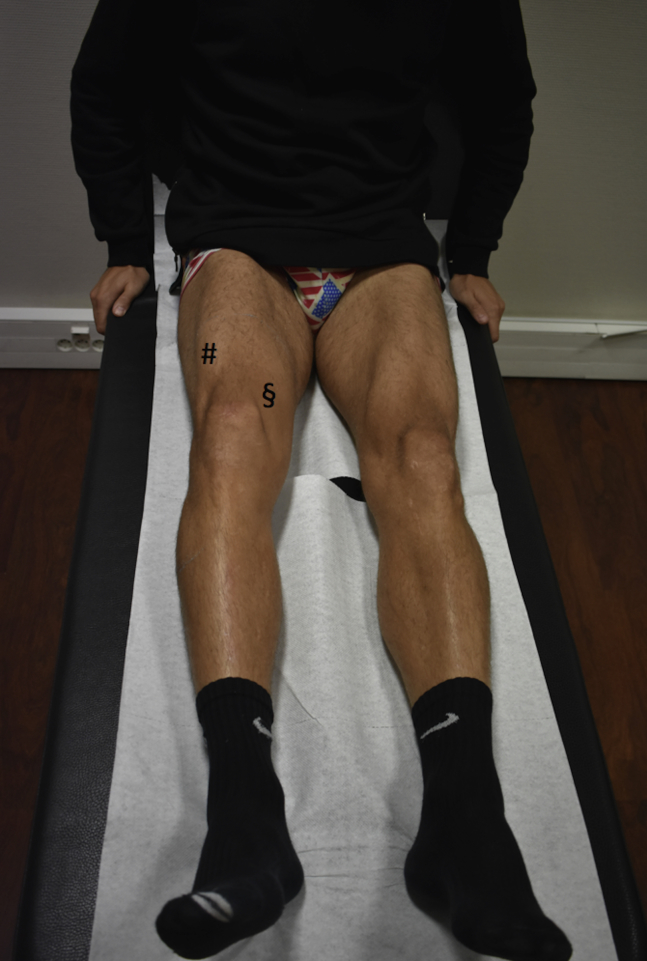
Right quadriceps inactivation with lack of vastus medialis contraction (section sign) and active knee extension deficit. The rectus femoris contraction (pound sign) is maintained with active hip flexion.

Hamstring fatigue. The patient is asked to repetitively contract against resistance (A) and relax the hamstrings (B). To help fully relax the hamstrings, the practitioner should gently support the foot on its way down to the examination table. A right knee is shown with the patient in the prone position.

Full knee extension (asterisk) recovery after hamstring fatigue. A right knee is shown with the patient in the prone position.

Passive muscle contraction of quadriceps. The patient is requested to do a heel lift (arrow) and straighten the knee. The practitioner can facilitate the movement by holding the great toe. A right knee is shown with the patient in the supine position.

Active isometric muscle contraction of quadriceps. The patient is asked to contract the muscle without lifting the heel. To check the correct contraction of the muscle, the practitioner should palpate the patella to feel its proximal migration (arrow). A right knee is shown with the patient in the supine position.
References
-
- Allum R.L., Jones J.R. The locked knee. Injury. 1986;17:256–258. - PubMed
-
- Rice D.A., McNair P.J. Quadriceps arthrogenic muscle inhibition: Neural mechanisms and treatment perspectives. Semin Arthritis Rheum. 2010;40:250–266. - PubMed
-
- Shakespeare D.T., Rigby H.S. The bucket-handle tear of the meniscus. A clinical and arthrographic study. J Bone Joint Surg Br. 1983;65:383–387. - PubMed
-
- McHugh M.P., Tyler T.F., Gleim G.W., Nicholas S.J. Preoperative indicators of motion loss and weakness following anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 1998;27:407–411. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
