

Natural History of Vanishing White Matter
- PMID: 30014503
- PMCID: PMC6175238
- DOI: 10.1002/ana.25287
Natural History of Vanishing White Matter
Abstract
Objective: To comprehensively describe the natural history of vanishing white matter (VWM), aiming at improving counseling of patients/families and providing natural history data for future therapeutic trials.
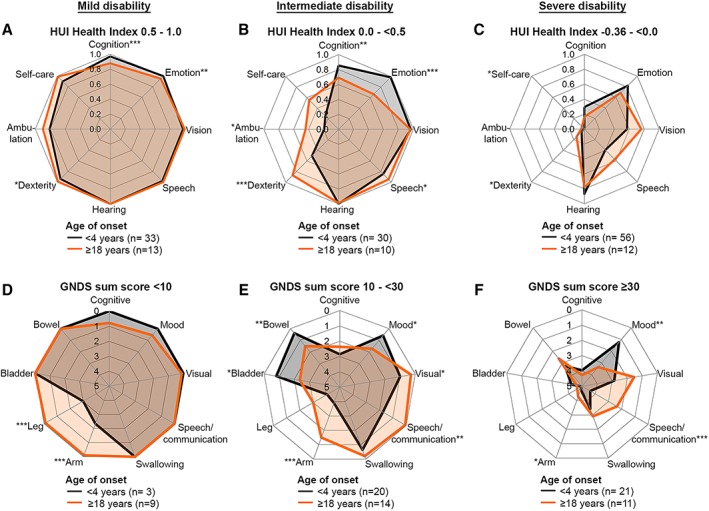
Methods: We performed a longitudinal multicenter study among 296 genetically confirmed VWM patients. Clinical information was obtained via disease-specific clinical questionnaire, Health Utilities Index and Guy's Neurological Disability Scale assessments, and chart review.
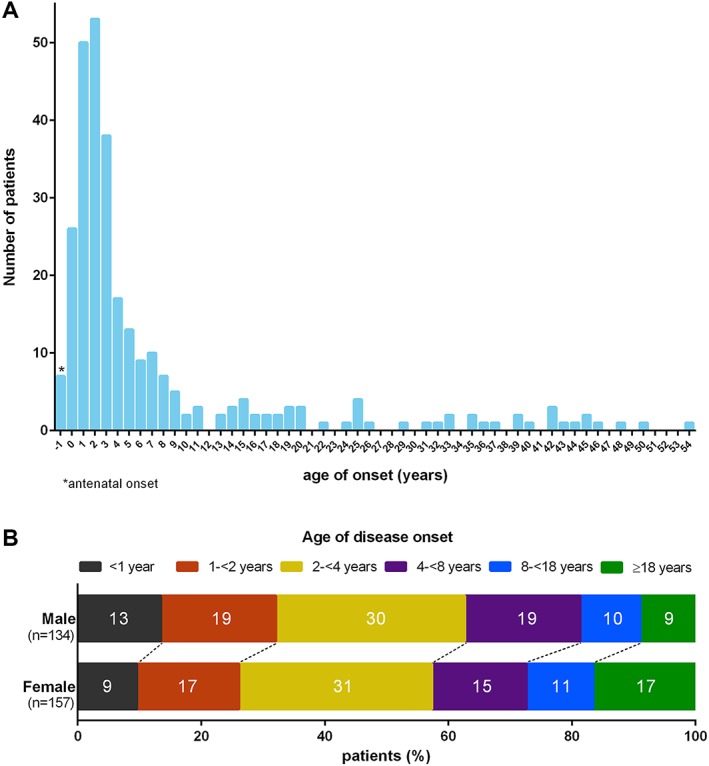
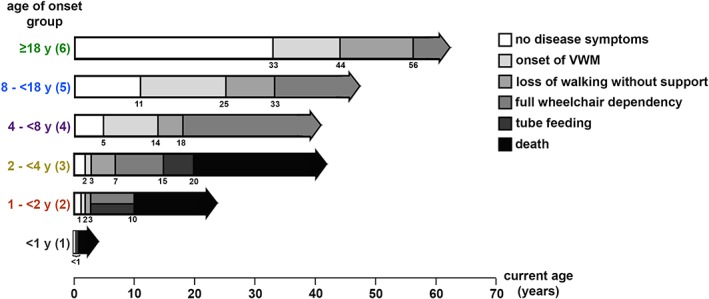
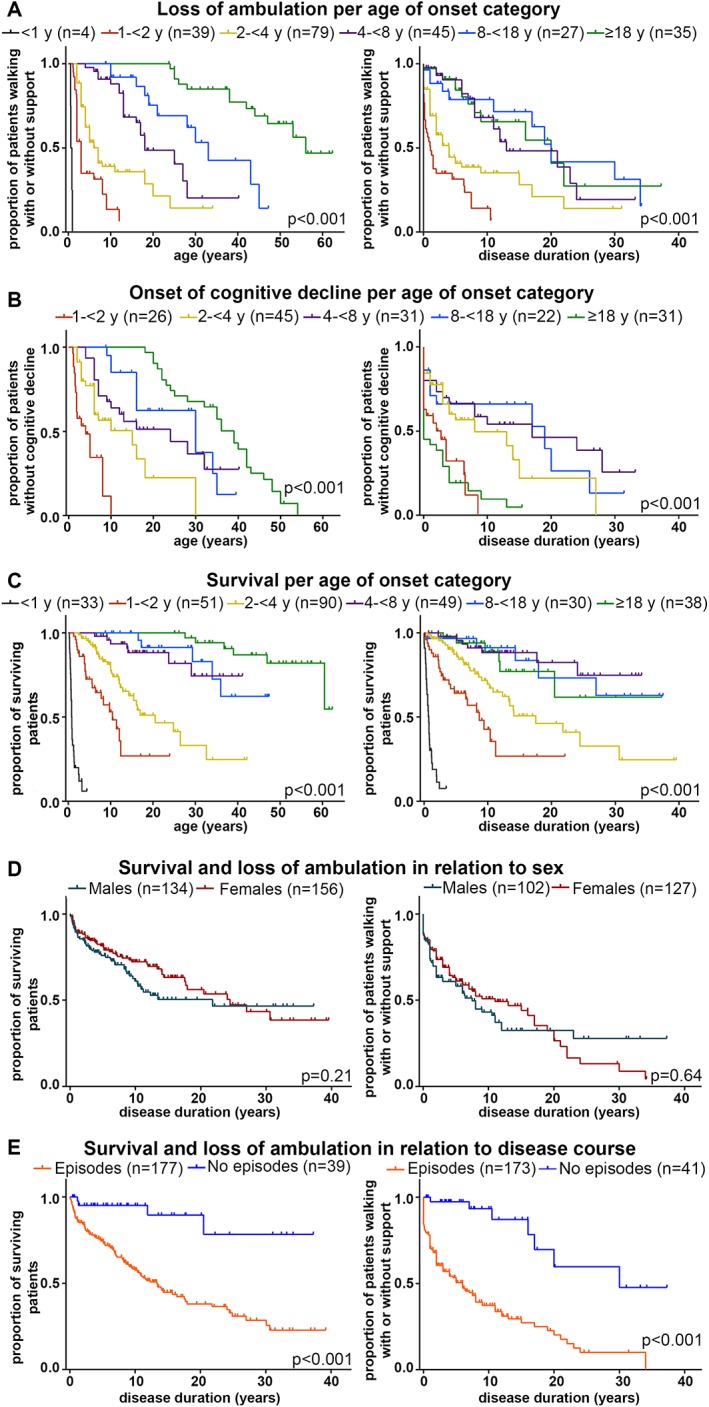
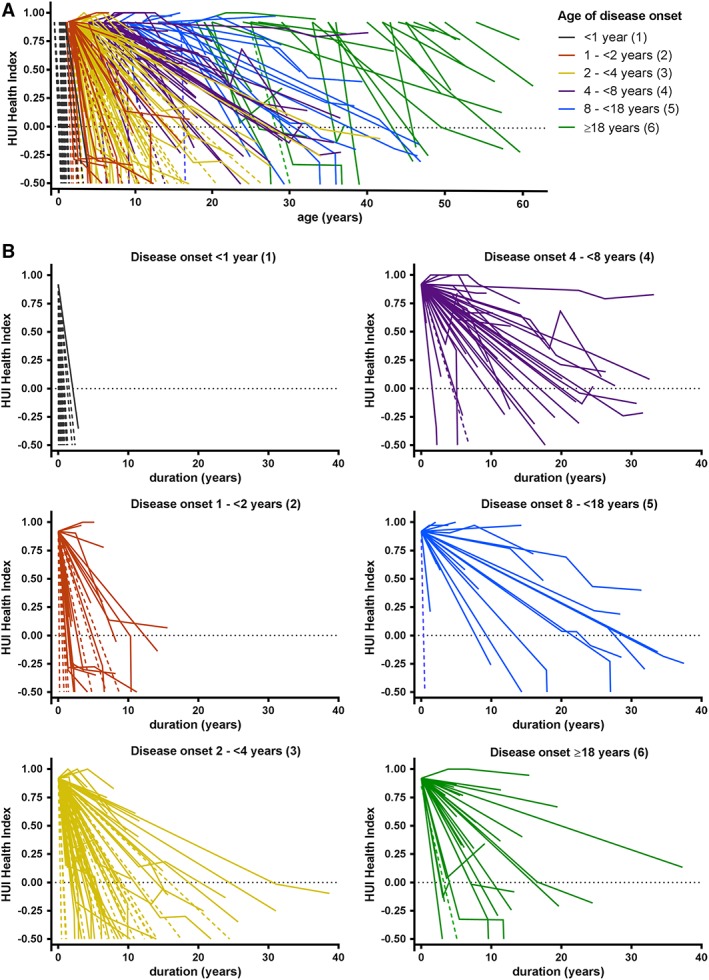
Results: First disease signs occurred at a median age of 3 years (mode = 2 years, range = before birth to 54 years); 60% of patients were symptomatic before the age of 4 years. The nature of the first signs varied for different ages of onset. Overall, motor problems were the most common presenting sign, especially in children. Adolescent and adult onset patients were more likely to exhibit cognitive problems early after disease onset. One hundred two patients were deceased. Multivariate Cox regression analysis revealed a positive relation between age at onset and both preservation of ambulation and survival. Absence of stress-provoked episodes and absence of seizures predicted more favorable outcome. In patients with onset before 4 years, earlier onset was associated with more severe disability and higher mortality. For onset from 4 years on, disease course was generally milder, with a wide variation in severity. There were no significant differences for sex or for the 5 eIF2B gene groups. The results confirm the presence of a genotype-phenotype correlation.
Interpretation: The VWM disease spectrum consists of a continuum with extremely wide variability. Age at onset is a strong predictor for disease course. Ann Neurol 2018;84:274-288.
© 2018 The Authors. Annals of Neurology published by Wiley Periodicals, Inc. on behalf of American Neurological Association.
Figures
References
-
- Schiffmann R, Moller JR, Trapp BD, et al. Childhood ataxia with diffuse central nervous system hypomyelination. Ann Neurol 1994;35:331–340. - PubMed
-
- van der Knaap MS, Barth PG, Gabreels FJ, et al. A new leukoencephalopathy with vanishing white matter. Neurology 1997;48:845–855. - PubMed
-
- van der Knaap MS, Kamphorst W, Barth PG, et al. Phenotypic variation in leukoencephalopathy with vanishing white matter. Neurology 1998;51:540–547. - PubMed
-
- Leegwater PA, Vermeulen G, Konst AA, et al. Subunits of the translation initiation factor eIF2B are mutant in leukoencephalopathy with vanishing white matter. Nat Genet 2001;29:383–388. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
