

A quantitative systems pharmacology (QSP) model for Pneumocystis treatment in mice
- PMID: 30016951
- PMCID: PMC6050661
- DOI: 10.1186/s12918-018-0603-9
A quantitative systems pharmacology (QSP) model for Pneumocystis treatment in mice
Erratum in
-
Correction to: A quantitative systems pharmacology (QSP) model for Pneumocystis treatment in mice.BMC Syst Biol. 2019 Aug 12;13(1):40. doi: 10.1186/s12918-019-0708-9. BMC Syst Biol. 2019. PMID: 31405372 Free PMC article.
Abstract
Background: The yeast-like fungi Pneumocystis, resides in lung alveoli and can cause a lethal infection known as Pneumocystis pneumonia (PCP) in hosts with impaired immune systems. Current therapies for PCP, such as trimethoprim-sulfamethoxazole (TMP-SMX), suffer from significant treatment failures and a multitude of serious side effects. Novel therapeutic approaches (i.e. newly developed drugs or novel combinations of available drugs) are needed to treat this potentially lethal opportunistic infection. Quantitative Systems Pharmacological (QSP) models promise to aid in the development of novel therapies by integrating available pharmacokinetic (PK) and pharmacodynamic (PD) knowledge to predict the effects of new treatment regimens.
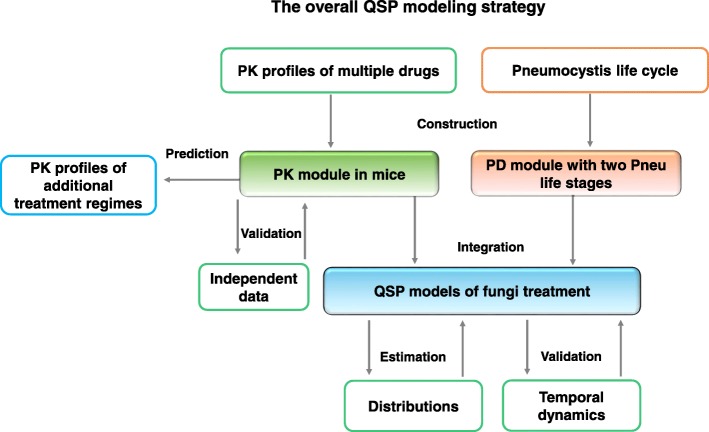
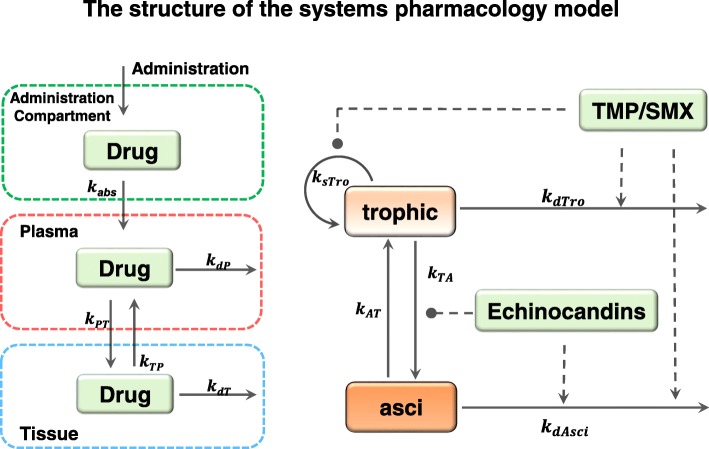
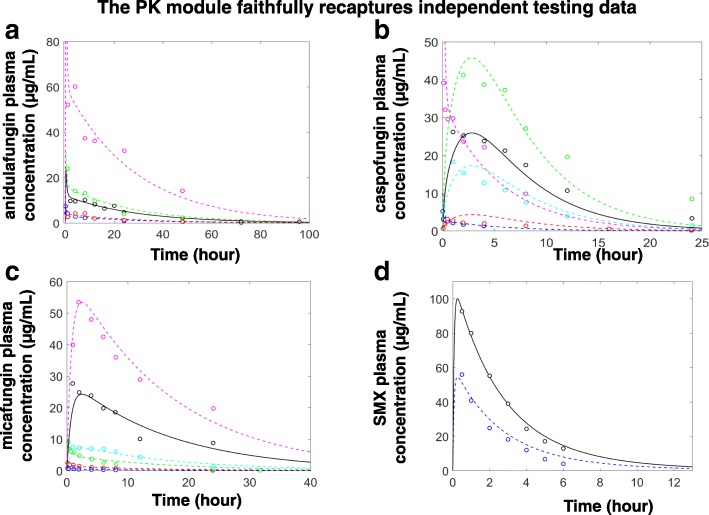
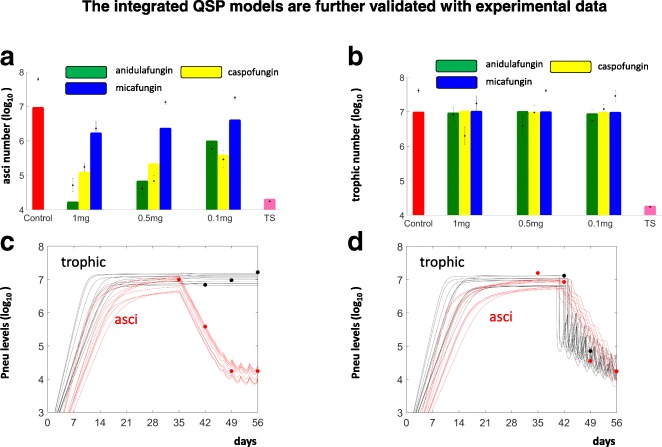
Results: In this work, we constructed and independently validated PK modules of a number of drugs with available pharmacokinetic data. Characterized by simple structures and well constrained parameters, these PK modules could serve as a convenient tool to summarize and predict pharmacokinetic profiles. With the currently accepted hypotheses on the life stages of Pneumocystis, we also constructed a PD module to describe the proliferation, transformation, and death of Pneumocystis. By integrating the PK module and the PD module, the QSP model was constrained with observed levels of asci and trophic forms following treatments with multiple drugs. Furthermore, the temporal dynamics of the QSP model were validated with corresponding data.
Conclusions: We developed and validated a QSP model that integrates available data and promises to facilitate the design of future therapies against PCP.
Keywords: Infectious disease; Pneumocystis - systems biology - quantitative systems pharmacology.
Conflict of interest statement
Ethics approval and consent to participate
The animal protocols used for this study were reviewed and approved by the University of Cincinnati’s IACUC committee and the Cincinnati Veterans Affairs Medical Center IACUC; protocols UC 12–05–03-01 and ACORP#15–02–25-01, respectively. Both committees adhere to the 8th edition of the “
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
