

Radiotherapy of Glioblastoma 15 Years after the Landmark Stupp's Trial: More Controversies than Standards?
- PMID: 30018514
- PMCID: PMC6043880
- DOI: 10.2478/raon-2018-0023
Radiotherapy of Glioblastoma 15 Years after the Landmark Stupp's Trial: More Controversies than Standards?
Abstract
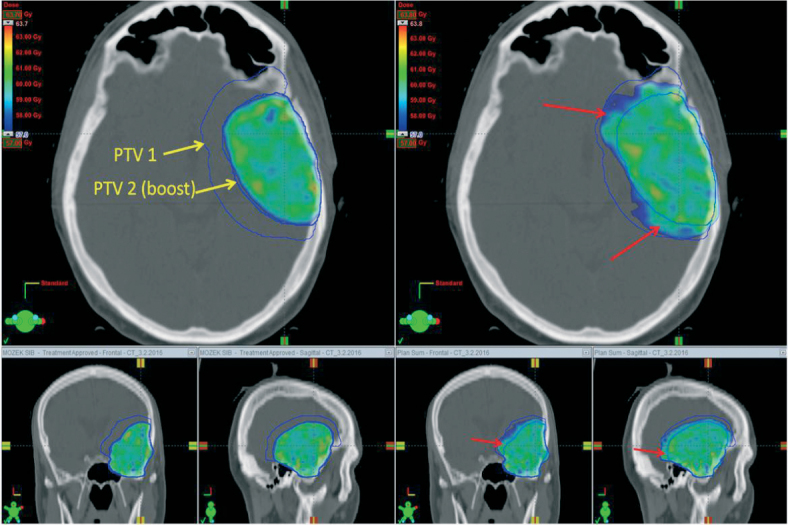
Background: The current standard of care of glioblastoma, the most common primary brain tumor in adults, has remained unchanged for over a decade. Nevertheless, some improvements in patient outcomes have occurred as a consequence of modern surgery, improved radiotherapy and up-to-date management of toxicity. Patients from control arms (receiving standard concurrent chemoradiotherapy and adjuvant chemotherapy with temozolomide) of recent clinical trials achieve better outcomes compared to the median survival of 14.6 months reported in Stupp's landmark clinical trial in 2005. The approach to radiotherapy that emerged from Stupp's trial, which continues to be a basis for the current standard of care, is no longer applicable and there is a need to develop updated guidelines for radiotherapy within the daily clinical practice that address or at least acknowledge existing controversies in the planning of radiotherapy.The goal of this review is to provoke critical thinking about potentially controversial aspects in the radiotherapy of glioblastoma, including among others the issue of target definitions, simultaneously integrated boost technique, and hippocampal sparing.
Conclusions: In conjunction with new treatment approaches such as tumor-treating fields (TTF) and immunotherapy, the role of adjuvant radiotherapy will be further defined. The personalized approach in daily radiotherapy practice is enabled with modern radiotherapy systems.
Keywords: controversy; glioblastoma; radiation therapy; radiotherapy dosage; target volumes.
Figures
References
-
- Malmström A, Grønberg BH, Marosi C, Stupp R, Frappaz D, Schultz H. et al. Temozolomide versus standard 6-week radiotherapy versus hypofractionated radiotherapy in patients older than 60 years with glioblastoma: the Nordic randomised, phase 3 trial. Lancet Oncol. 2012;13:916–26. doi: 10.1016/S1470-2045(12)70265-6. - DOI - PubMed
-
- Hegi ME, Diserens AC, Gorlia T, Hamou MF, de Tribolet N, Weller M. et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med. 2005;352:997–1003. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
