

A randomized clinical trial of the efficacy and safety of sitagliptin compared with dapagliflozin in patients with type 2 diabetes mellitus and mild renal insufficiency: The CompoSIT-R study
- PMID: 30019498
- PMCID: PMC6283039
- DOI: 10.1111/dom.13473
A randomized clinical trial of the efficacy and safety of sitagliptin compared with dapagliflozin in patients with type 2 diabetes mellitus and mild renal insufficiency: The CompoSIT-R study
Abstract
Aim: To compare the efficacy and safety of the dipeptidyl peptidase-4 inhibitor sitagliptin with the sodium-glucose transporter-2 inhibitor dapagliflozin in patients with type 2 diabetes and mild renal insufficiency.
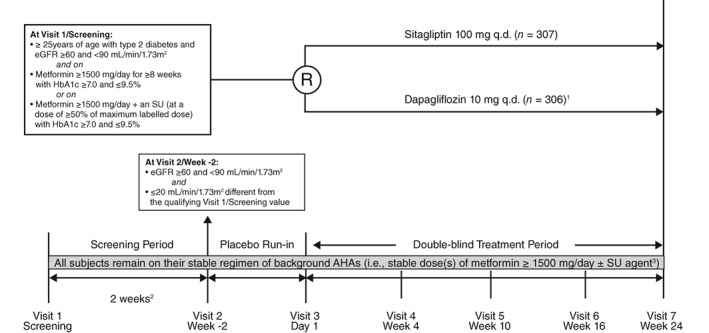
Materials and methods: Patients with HbA1c ≥7.0 to ≤9.5% (≥53 to ≤80 mmol/mol) and estimated glomerular filtration rate ≥60 to <90 mL/min/1.73m2 on metformin (≥1500 mg/d) ± sulfonylurea were randomized to sitagliptin 100 mg (n = 307) or dapagliflozin 5 mg titrated to 10 mg (n = 306) once daily for 24 weeks. A longitudinal data analysis model was used to test the primary hypothesis that sitagliptin is non-inferior to dapagliflozin in reducing HbA1c at Week 24, with superiority to be tested if non-inferiority is met. ClinicalTrials.gov NCT02532855.
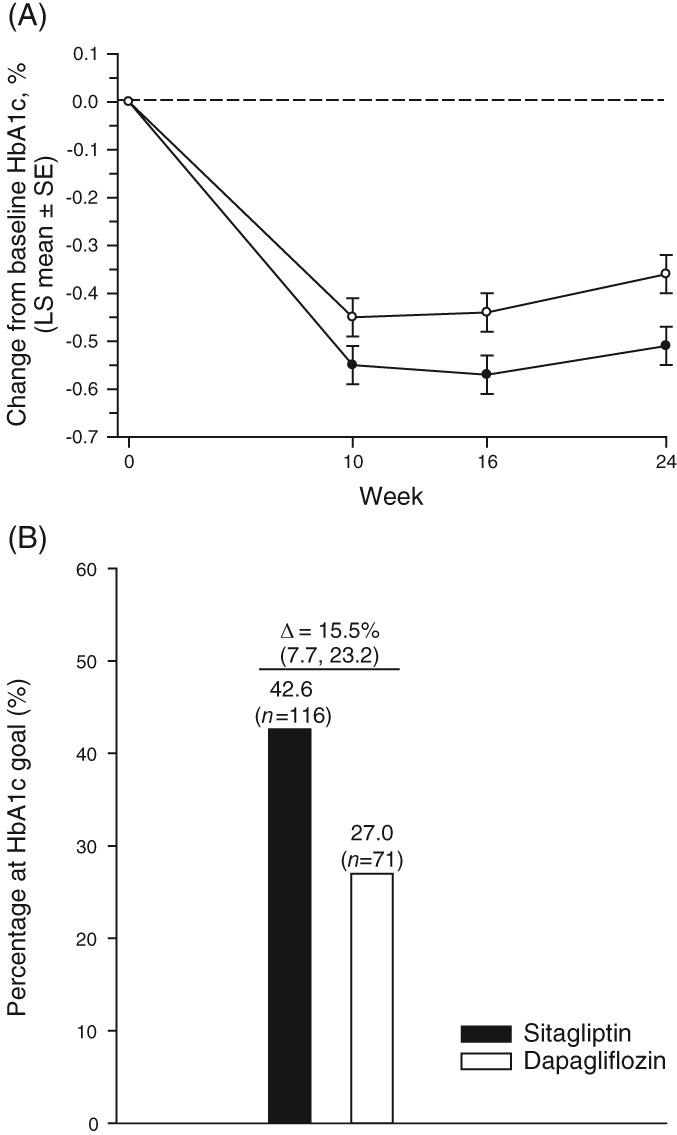
Results: Baseline mean HbA1c (% [mmol/mol]) was 7.7 (60.9) and 7.8 (61.2), and mean eGFR (mL/min/1.73m2 ) was 79.4 and 76.9 for the sitagliptin and dapagliflozin groups, respectively. After 24 weeks, the between-group difference in least squares mean (95% CI) changes from baseline in HbA1c was -0.15% (-0.26, -0.04) (-1.67 mmol/mol [-2.86, -0.48]), P = 0.006, meeting the prespecified criteria for declaring both non-inferiority and superiority of sitagliptin versus dapagliflozin. The HbA1c goal of <7% (<53 mmol/mol) was met by 43% (sitagliptin) and 27% (dapagliflozin) of patients. No meaningful between-group difference was observed in a pre-specified analysis of 2-hour incremental postprandial glucose excursion. A review of adverse events (AEs) was notable for a lower incidence of drug-related AEs with sitagliptin compared with dapagliflozin.
Conclusions: In patients with type 2 diabetes, mild renal insufficiency and inadequate glycaemic control on metformin ± sulfonylurea, sitagliptin treatment resulted in greater improvement in glycaemic control compared with dapagliflozin and was generally well tolerated.
Keywords: clinical trial; dapagliflozin; sitagliptin; type 2 diabetes.
© 2018 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
J. M., Z. Z., R. L. H. L., E. A. O., K. D. K., S. S. E. and A. R. are employees of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, and may hold stock and/or stock options in the company. R. S. has no conflicts of interest to declare.
Figures
References
-
- Deacon CF. A review of dipeptidyl peptidase‐4 inhibitors. Hot topics from randomized controlled trials. Diabetes Obes Metab. 2018;20(Suppl 1):34‐46. - PubMed
-
- Arnouts P, Bolignano D, Nistor I, et al. Glucose‐lowering drugs in patients with chronic kidney disease: a narrative review on pharmacokinetic properties. Nephrol Dial Transplant. 2014;29:1284‐1300. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
