

Combined use of topical intraarticular tranexamic acid and rivaroxaban in total knee arthroplasty safely reduces blood loss, transfusion rates, and wound complications without increasing the risk of thrombosis
- PMID: 30021575
- PMCID: PMC6052595
- DOI: 10.1186/s12891-018-2151-2
Combined use of topical intraarticular tranexamic acid and rivaroxaban in total knee arthroplasty safely reduces blood loss, transfusion rates, and wound complications without increasing the risk of thrombosis
Abstract
Background: Blood loss and deep vein thrombosis (DVT) are important complications after total knee arthroplasty (TKA). Topical tranexamic acid (TXA) effectively reduces wound bleeding but may elevate the risk of DVT. In contrast, rivaroxaban potently prevents DVT but has been associated with bleeding complications. The simultaneous use of topical TXA and rivaroxaban in TKA has not been much investigated.
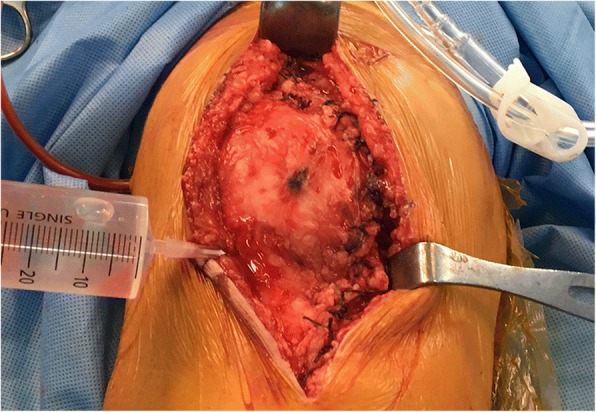
Methods: A retrospective cohort study was conducted with two consecutive groups of patients who underwent TKA. Intraoperatively, one group (RVTX group) received topical, intraarticular TXA, while the other (RV group) did not. Both groups were administered rivaroxaban postoperatively for 14 days and underwent Doppler ultrasound for DVT screening. After propensity score matching, both groups consisted of 52 patients (104 patients in total) and were compared regarding total drain output, nadir haemoglobin (Hb), maximum Hb decrease, calculated total blood loss, transfusion rate, and incidence of DVT and wound complications.
Results: Both groups showed no significant differences in the propensity-matched variables of age, sex, body mass index, American Society of Anesthesiologists physical status score, and preoperative Hb. The RVTX group showed a significantly higher nadir Hb (p < 0.001), lower drain output (p < 0.001), Hb decrease (p = 0.015), total blood loss (p < 0.001), and rate of transfusion (p < 0.001) and fewer wound complications (p = 0.027). However, the incidence of DVT (p = 1.000) did not differ significantly between the two groups, and all cases were asymptomatic.
Conclusions: The combined use of intraarticular topical TXA with rivaroxaban in patients undergoing TKA is a safe and effective method to reduce blood loss, the need for transfusion, and wound complications without elevating the risk of DVT.
Keywords: Blood loss; Deep vein thrombosis; Rivaroxaban; Total knee replacement; Tranexamic acid; Transfusion; Wound complication.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Hallym University Kangnam Sacred Heart Hospital Institutional Review Board (IRB number: HUKSHH IRB 2017–10-010). Informed consent was waivered by the above IRB as the present retrospective cohort study involved already existing data and records at the time of investigation, and did not retain personal identifiers of the gathered information.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
