Cumulative childhood adversity and adult cardiometabolic disease: A meta-analysis
- PMID: 30024227
- PMCID: PMC6109976
- DOI: 10.1037/hea0000637
Cumulative childhood adversity and adult cardiometabolic disease: A meta-analysis
Abstract
Objective: Adverse childhood experiences may be associated with cardiometabolic morbidity and mortality in adulthood. There is heterogeneity in this literature regarding the type of items in cumulative adversity indices, sample sizes, demographics, and covariates. The present review used quantitative meta-analysis to examine this association and potential moderators.
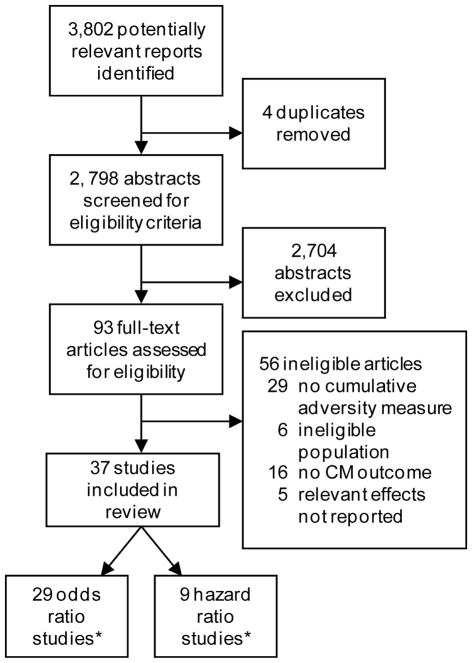
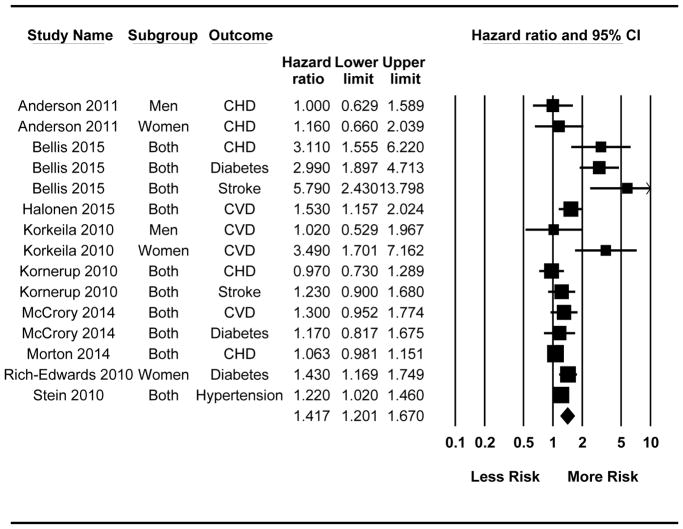
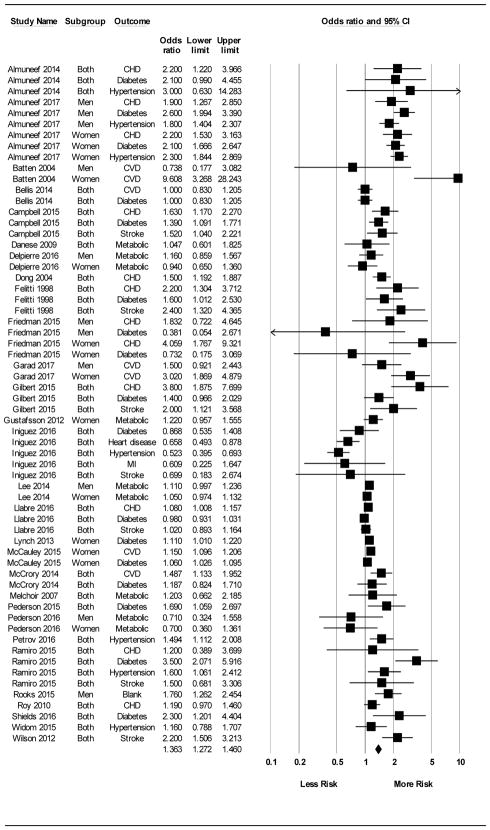
Method: Included studies had a measure of cumulative adversity (an index of at least 2 adverse childhood experiences from age 0 to 18) and a measure of cardiometabolic disease: cardiovascular disease (CVD) clinical outcomes (hypertension, coronary heart disease, ischemic heart disease, myocardial infarction, stroke, cerebrovascular disease) and metabolic outcomes (diabetes, metabolic syndrome) at age 18 or older. Given different interpretations of odds ratios (OR) versus hazard ratios (HR), effects were pooled separately. Overall, 9 HR studies (15 effects) based on 179,612 participants and 29 OR studies (62 effects) based on 247,393 participants were included.
Results: On the basis of retrospectively assessed adversity, combined studies showed a significant estimated effect of cumulative childhood adversity on adult cardiometabolic disease (HR = 1.42, 95% CI [1.20, 1.67]; OR = 1.36 [1.27, 1.46]). Results varied somewhat by type of cardiometabolic disease, analytic strategy, and number and type of covariates.
Conclusions: The literature suggests that cumulative childhood adversity is modestly related to adult cardiometabolic disease, with effects somewhat stronger for CVD clinical outcomes. The absence of a consistent operational and conceptual definition of adversity and paucity of prospective designs temper the conclusions. It is time for further evaluation of the types and timing of childhood events that have maximal impact on adult cardiometabolic disease. (PsycINFO Database Record
(c) 2018 APA, all rights reserved).
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources