

Comparison of clinical and radiological outcomes between modified Gallie graft fusion-wiring technique and posterior cervical screw constructs for Type II odontoid fractures
- PMID: 30024518
- PMCID: PMC6086456
- DOI: 10.1097/MD.0000000000011452
Comparison of clinical and radiological outcomes between modified Gallie graft fusion-wiring technique and posterior cervical screw constructs for Type II odontoid fractures
Abstract
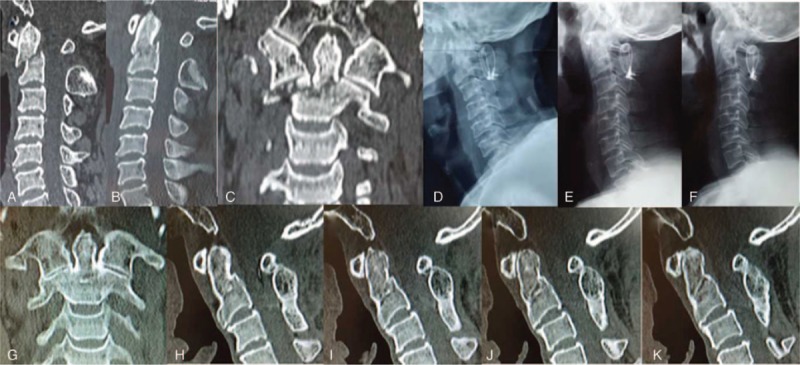
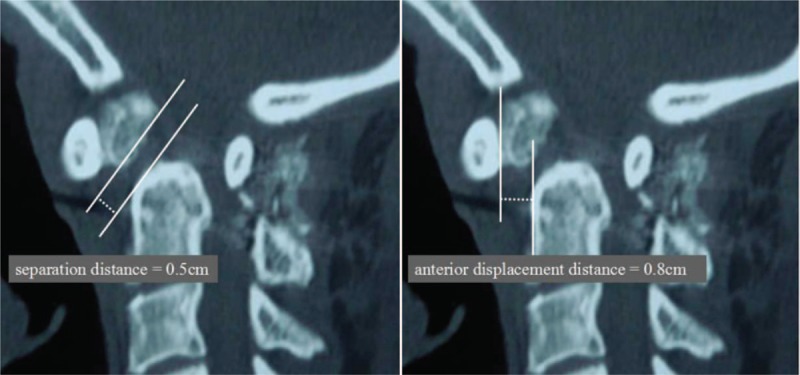
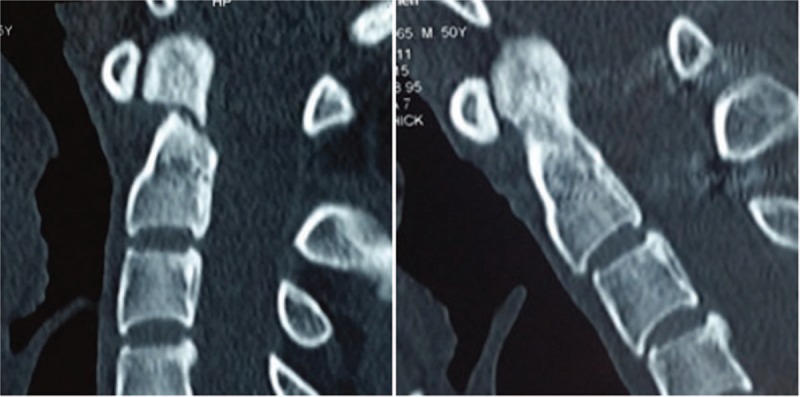
The aim of this study was to compare clinical and radiological outcomes between modified Gallie graft fusion-wiring technique and posterior cervical screw constructs for Type II odontoid fractures, and hope to provide references in decision making and surgical planning for both spinal surgeons and surgically treated patients.This is a retrospective study. By retrieving the medical records from January 2005 to July 2015 in our hospital, 53 Type II odontoid fracture patients were reviewed. According to the instrumentation type, patients were divided into 2 groups: Wiring group and Screw group. Three categorized factors were analyzed statistically: patient characteristics: age, body mass index, preoperative neurological status, duration, complicated injuries; surgical variables: surgery time, blood loss, vertebral artery injury, spinal cord or nerve root injury, major systemic complications, wound infection, pain at the bone donor area, instrumentation failure, revision rate; and radiographic parameters: preoperative and final follow-up data of C0-2 curvature, C2-7 curvature, C2-C7 sagittal vertical axis, C7 slope, fracture classification, separation, and displacement of odontoid fracture, fusion rate. An additional comparison of surgical outcomes was done, including patient satisfaction, visual analog scale score for neck pain, neck stiffness, medical expense.There was no statistically significant difference between the 2 groups in patient characteristics of age, sex, body mass index, preoperative neurological status, duration, and complicated injuries. No statistically significant difference was noted in surgical variables of blood loss, vertebral artery injury, spinal cord or nerve root injury, major systemic complications, wound infection, bone harvested zone pain, instrumentation failure, revision rate. The surgery time was shorter in Wiring group than that in Screw group, with a statistically significant difference. We noted no significant difference between the 2 groups when comparing radiographic parameters of preoperative and final follow-up data of C0-2 curvature, C2-C7 sagittal vertical axis, fracture classification, the separation and displacement of odontoid fracture, and fusion rate. Although we noted no significant difference in preoperative C2-7 curvature and C7 slope, the final follow-up data showed that C2-7 curvature and C7 slope were smaller in Wiring group than that in Screw group. We noted no significant difference in visual analog scale score, neck stiffness, and neurological status at final follow-up. The medical expense was less in Wiring group; the patient satisfaction was lower in the Wiring group than that in the Screw group.The modified Gallie graft fusion-wiring technique provided solid fusion and stabilization for patients with Type II odontoid fractures, Gallie graft fusion-wiring resulted in less surgery time, less medical expense, but lower patient satisfaction when compared with the posterior cervical screw constructs.
Conflict of interest statement
The authors have no conflicts of interest.
Figures




References
-
- Wang H, Wang Q, Ma L, et al. Predisposing factors of fracture nonunion after posterior C1 lateral mass screws combined with C2 pedicle/laminar screw fixation for Type II odontoid fracture. World Neurosurg 2018;109:e417–25. - PubMed
-
- Ishak B, Schneider T, Gimmy V, et al. Early complications, morbidity, and mortality in octogenarians and nonagenarians undergoing posterior intra-operative spinal navigation- based C1/2 fusion for Type II odontoid process fractures. J Neurotrauma 2017;34:3326–35. - PubMed
-
- Subach BR, Morone MA, Haid RW, Jr, et al. Management of acute odontoid fractures with single-screw anterior fixation. Neurosurgery 1999;45:812–9. - PubMed
-
- Joaquim AF, Patel AA. Surgical treatment of Type II odontoid fractures: anterior odontoid screw fixation or posterior cervical instrumented fusion? Neurosurg Focus 2015;38:E11. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
