

CPX-351 (cytarabine and daunorubicin) Liposome for Injection Versus Conventional Cytarabine Plus Daunorubicin in Older Patients With Newly Diagnosed Secondary Acute Myeloid Leukemia
- PMID: 30024784
- PMCID: PMC6127025
- DOI: 10.1200/JCO.2017.77.6112
CPX-351 (cytarabine and daunorubicin) Liposome for Injection Versus Conventional Cytarabine Plus Daunorubicin in Older Patients With Newly Diagnosed Secondary Acute Myeloid Leukemia
Abstract
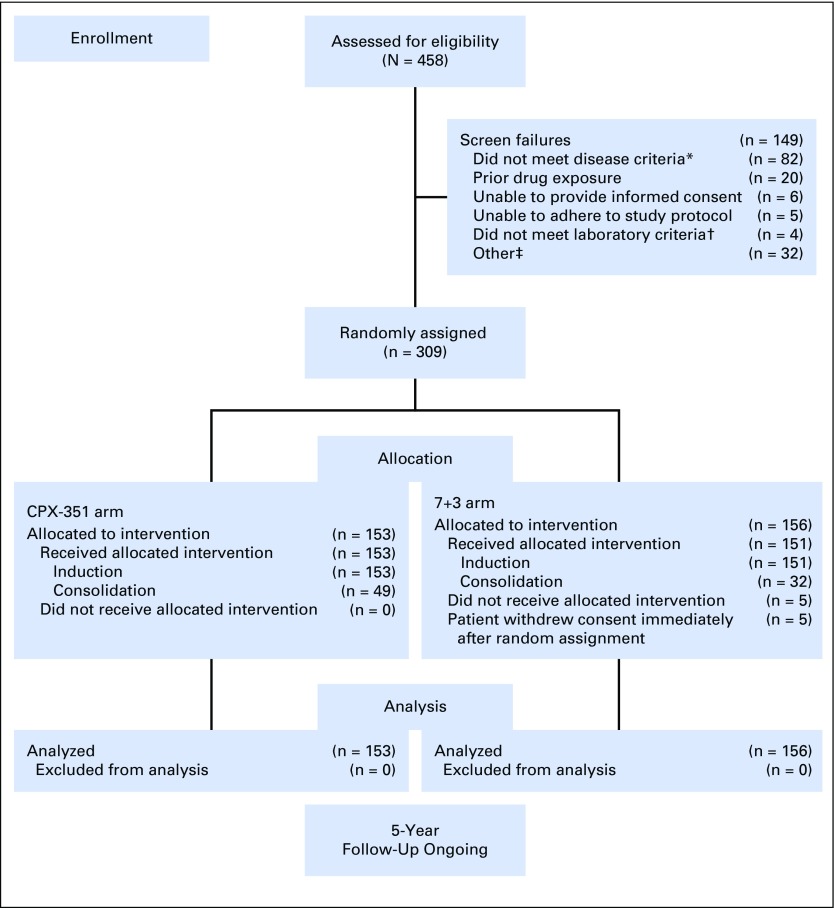
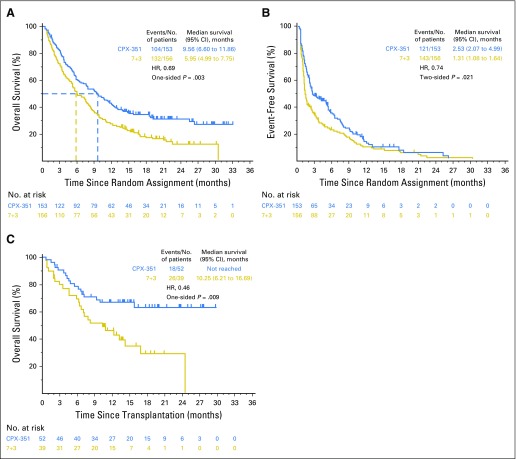
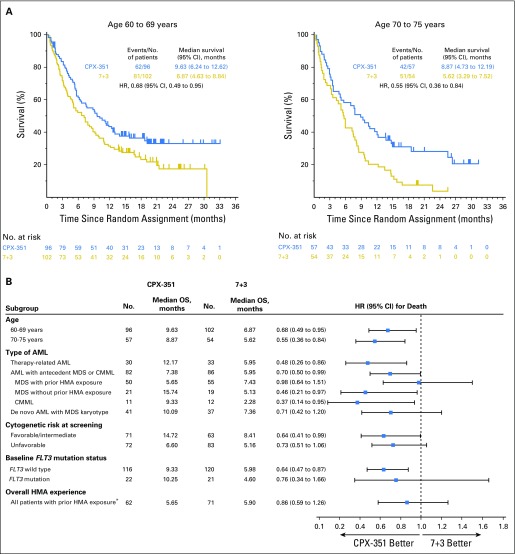
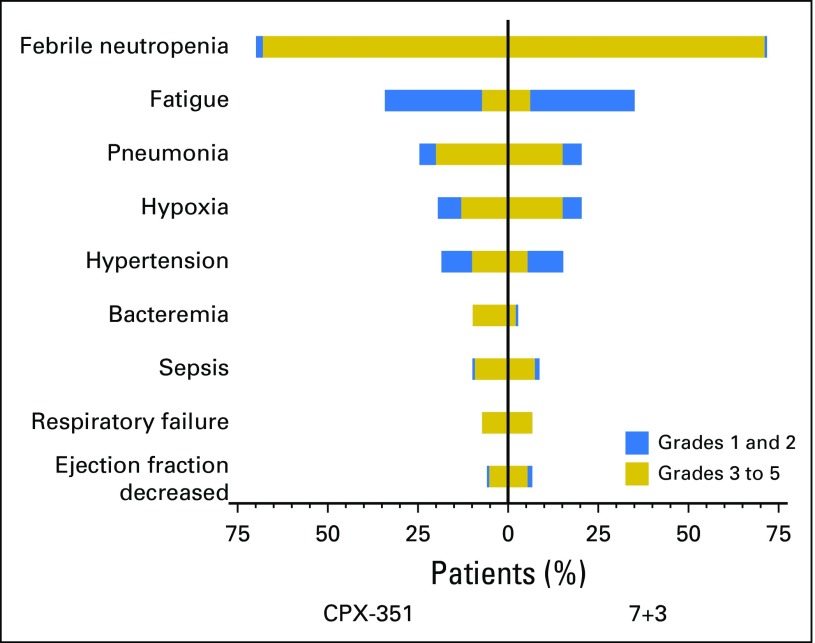
Purpose CPX-351 is a dual-drug liposomal encapsulation of cytarabine and daunorubicin that delivers a synergistic 5:1 drug ratio into leukemia cells to a greater extent than normal bone marrow cells. Prior clinical studies demonstrated a sustained drug ratio and exposure in vivo and prolonged survival versus standard-of-care cytarabine plus daunorubicin chemotherapy (7+3 regimen) in older patients with newly diagnosed secondary acute myeloid leukemia (sAML). Patients and Methods In this open-label, randomized, phase III trial, 309 patients age 60 to 75 years with newly diagnosed high-risk/sAML received one to two induction cycles of CPX-351 or 7+3 followed by consolidation therapy with a similar regimen. The primary end point was overall survival. Results CPX-351 significantly improved median overall survival versus 7+3 (9.56 v 5.95 months; hazard ratio, 0.69; 95% CI, 0.52 to 0.90; one-sided P = .003). Overall remission rate was also significantly higher with CPX-351 versus 7+3 (47.7% v 33.3%; two-sided P = .016). Improved outcomes were observed across age-groups and AML subtypes. The incidences of nonhematologic adverse events were comparable between arms, despite a longer treatment phase and prolonged time to neutrophil and platelet count recovery with CPX-351. Early mortality rates with CPX-351 and 7+3 were 5.9% and 10.6% (two-sided P = .149) through day 30 and 13.7% and 21.2% (two-sided P = .097) through day 60. Conclusion CPX-351 treatment is associated with significantly longer survival compared with conventional 7+3 in older adults with newly diagnosed sAML. The safety profile of CPX-351 was similar to that of conventional 7+3 therapy.
Trial registration: ClinicalTrials.gov NCT01696084.
Figures
Comment in
-
Benefit of nanomedicine confirmed in sAML.Nat Rev Clin Oncol. 2018 Oct;15(10):591. doi: 10.1038/s41571-018-0080-5. Nat Rev Clin Oncol. 2018. PMID: 30065313 No abstract available.
References
-
- Vardiman JW, Thiele J, Arber DA, et al. : The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: Rationale and important changes. Blood 114:937-951, 2009 - PubMed
-
- Granfeldt Østgård LS, Medeiros BC, Sengeløv H, et al. : Epidemiology and clinical significance of secondary and therapy-related acute myeloid leukemia: A national population-based cohort study. J Clin Oncol 33:3641-3649, 2015 - PubMed
-
- Miesner M, Haferlach C, Bacher U, et al. : Multilineage dysplasia (MLD) in acute myeloid leukemia (AML) correlates with MDS-related cytogenetic abnormalities and a prior history of MDS or MDS/MPN but has no independent prognostic relevance: A comparison of 408 cases classified as “AML not otherwise specified” (AML-NOS) or “AML with myelodysplasia-related changes” (AML-MRC). Blood 116:2742-2751, 2010 - PubMed
-
- Hulegårdh E, Nilsson C, Lazarevic V, et al. : Characterization and prognostic features of secondary acute myeloid leukemia in a population-based setting: A report from the Swedish Acute Leukemia Registry. Am J Hematol 90:208-214, 2015 - PubMed
-
- Leith CP, Kopecky KJ, Godwin J, et al. : Acute myeloid leukemia in the elderly: Assessment of multidrug resistance (MDR1) and cytogenetics distinguishes biologic subgroups with remarkably distinct responses to standard chemotherapy. A Southwest Oncology Group study. Blood 89:3323-3329, 1997 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
