

Structural remodeling and conduction velocity dynamics in the human left atrium: Relationship with reentrant mechanisms sustaining atrial fibrillation
- PMID: 30026014
- PMCID: PMC6317307
- DOI: 10.1016/j.hrthm.2018.07.019
Structural remodeling and conduction velocity dynamics in the human left atrium: Relationship with reentrant mechanisms sustaining atrial fibrillation
Abstract
Background: Rate-dependent conduction velocity (CV) slowing is associated with atrial fibrillation (AF) initiation and reentrant mechanisms.
Objective: The purpose of this study was to assess the relationship between bipolar voltage, CV dynamics, and AF drivers.
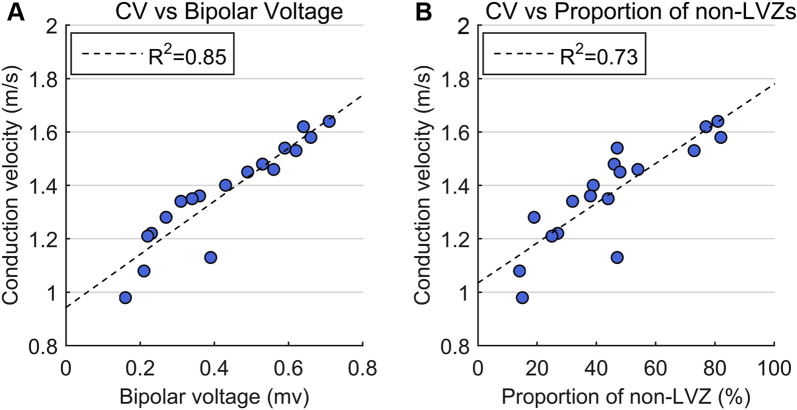
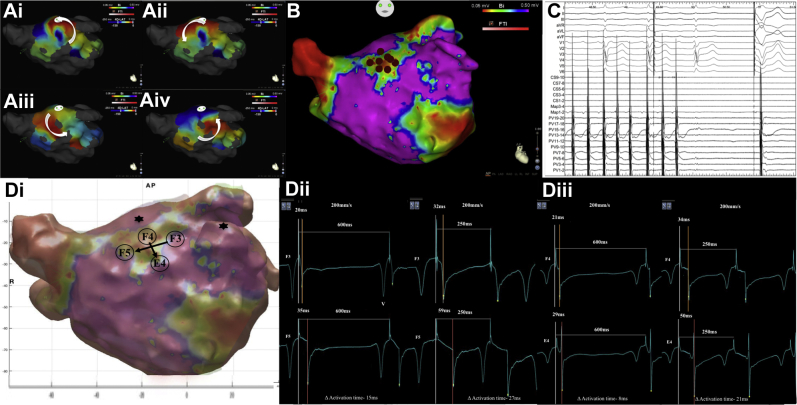
Methods: Patients undergoing catheter ablation for persistent AF (<24 months) were enrolled. Unipolar electrograms were recorded with a 64-pole basket catheter during atrial pacing at 4 pacing intervals (PIs) during sinus rhythm. CVs were measured between pole pairs along the wavefront path and correlated with underlying bipolar voltage. CV dynamics within low-voltage zones (LVZs <0.5 mV) were compared to those of non-LVZs (≥0.5 mV) and were correlated to driver sites mapped using CARTOFINDER (Biosense Webster).
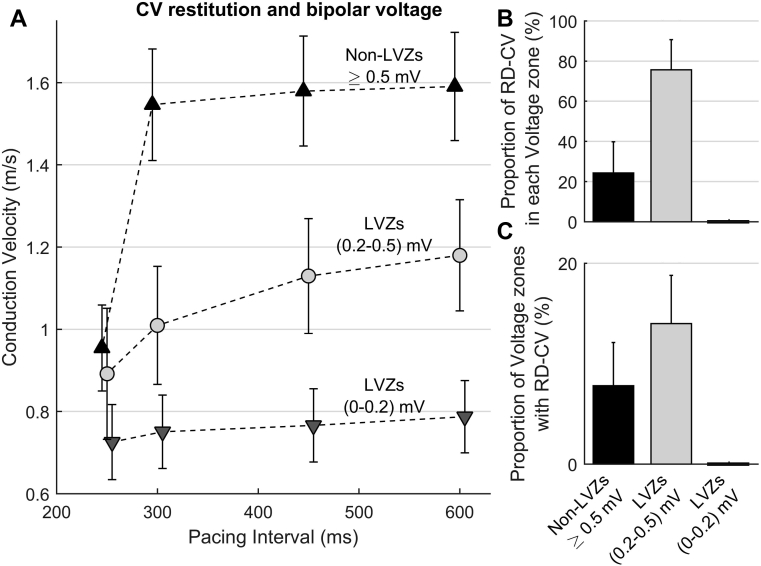
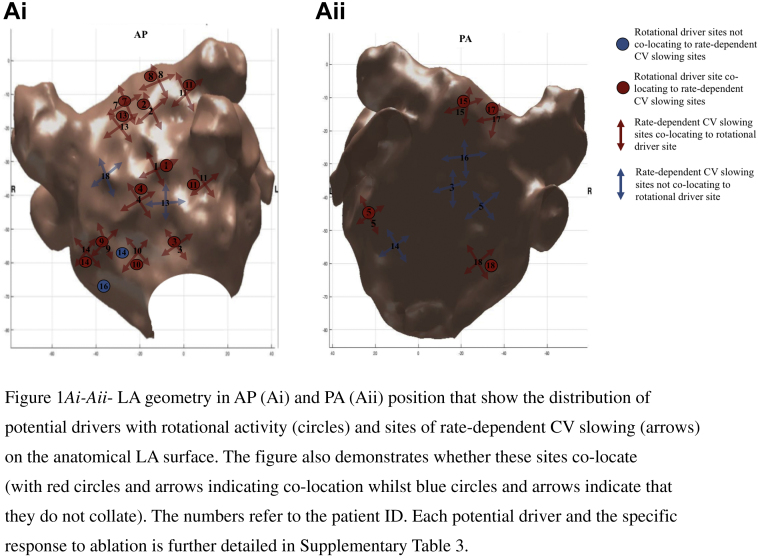
Results: Eighteen patients were included (age 62 ± 10 years). Mean CV at 600 ms was 1.59 ± 0.13 m/s in non-LVZs vs 0.98 ± 0.23 m/s in LVZs (P <.001). CV decreased incrementally over all 4 PIs in LVZs, whereas in non-LVZs a substantial decrease in CV was only seen between PIs 300-250 ms (0.59 ± 0.09 m/s; P <.001). Rate-dependent CV slowing sites measurements, defined as exhibiting CV reduction ≥20% more than the mean CV reduction seen between PIs 600-250 ms for that voltage zone, were predominantly in LVZs (0.2-0.5 mV; 75.6% ± 15.5%; P <.001). Confirmed rotational drivers were mapped to these sites in 94.1% of cases (sensitivity 94.1%, 95% CI 71.3%-99.9%; specificity 77.9%, 95% CI 74.9%-80.7%).
Conclusion: CV dynamics are determined largely by the extent of remodeling. Rate-dependent CV slowing sites are predominantly confined to LVZs (0.2-0.5 mV), and the resultant CV heterogeneity may promote driver formation in AF.
Keywords: Atrial fibrillation; Bipolar voltage; Conduction velocity; Drivers; Structural remodeling.
Crown Copyright © 2018. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Miyamoto K., Tsuchiya T., Narita S., Yamaguchi T., Nagamoto Y., Ando S., Hayashida K., Tanioka Y., Takahashi N. Bipolar electrogram amplitudes in the left atrium are related to local conduction velocity in patients with atrial fibrillation. Europace. 2009;11:1597–1605. - PubMed
-
- Yagishita A., Gimbel J.R., DE Oliveira S., Manyam H., Sparano D., Cakulev I., Mackall J., Arruda M. Long-term outcome of left atrial voltage-guided substrate ablation during atrial fibrillation: a novel adjunctive ablation strategy. J Cardiovasc Electrophysiol. 2017;28:147–155. - PubMed
-
- Koller M.L., Maier S.K., Gelzer A.R., Bauer W.R., Meesmann M., Gilmour R.F., Jr. Altered dynamics of action potential restitution and alternans in humans with structural heart disease. Circulation. 2005;112:1542–1548. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
