

Subacromial decompression versus diagnostic arthroscopy for shoulder impingement: randomised, placebo surgery controlled clinical trial
- PMID: 30026230
- PMCID: PMC6052435
- DOI: 10.1136/bmj.k2860
Subacromial decompression versus diagnostic arthroscopy for shoulder impingement: randomised, placebo surgery controlled clinical trial
Abstract
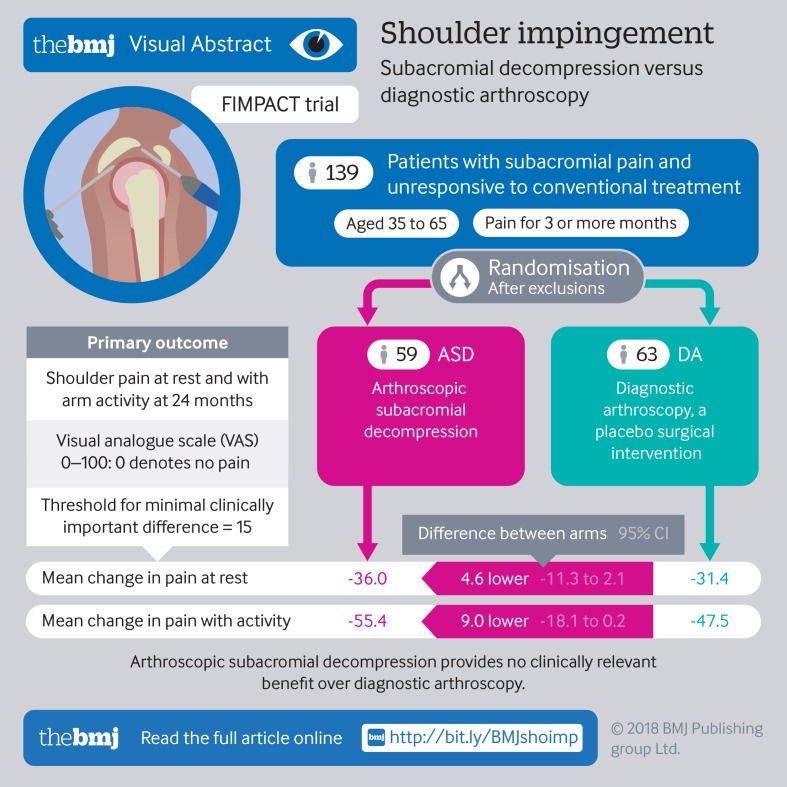
Objective: To assess the efficacy of arthroscopic subacromial decompression (ASD) by comparing it with diagnostic arthroscopy, a placebo surgical intervention, and with a non-operative alternative, exercise therapy, in a more pragmatic setting.
Design: Multicentre, three group, randomised, double blind, sham controlled trial.
Setting: Orthopaedic departments at three public hospitals in Finland.
Participants: 210 patients with symptoms consistent with shoulder impingement syndrome, enrolled from 1 February 2005 with two year follow-up completed by 25 June 2015.
Interventions: ASD, diagnostic arthroscopy (placebo control), and exercise therapy.
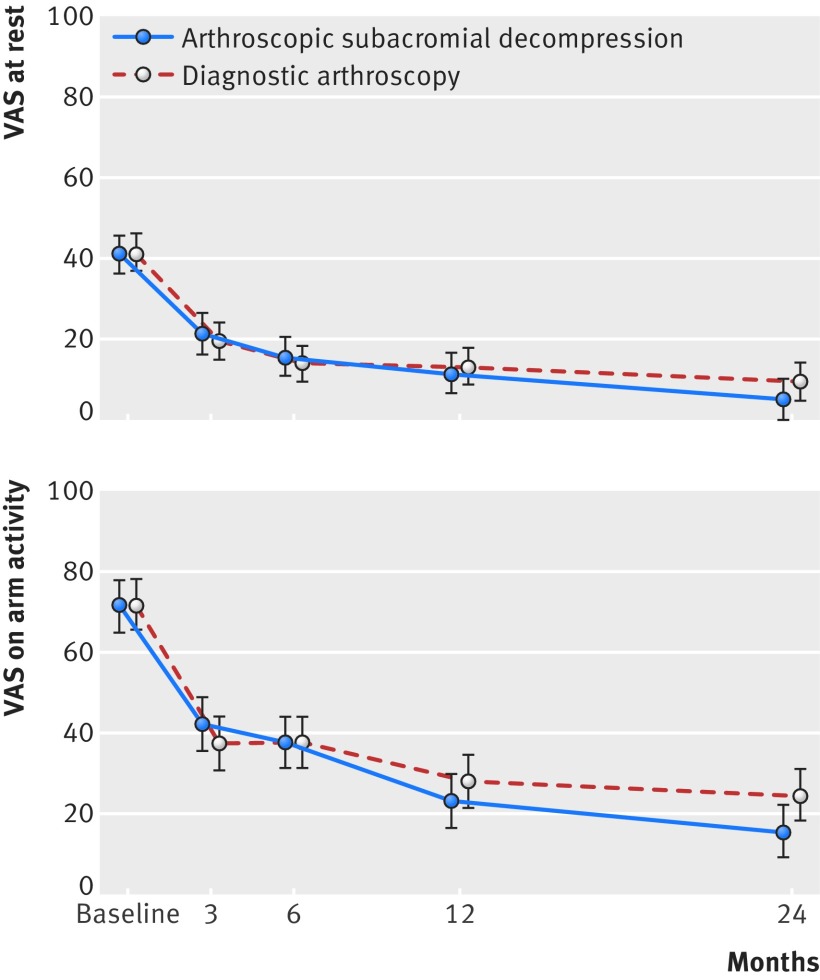
Main outcome measures: Shoulder pain at rest and on arm activity (visual analogue scale (VAS) from 0 to 100, with 0 denoting no pain), at 24 months. The threshold for minimal clinically important difference was set at 15.
Results: In the primary intention to treat analysis (ASD versus diagnostic arthroscopy), no clinically relevant between group differences were seen in the two primary outcomes at 24 months (mean change for ASD 36.0 at rest and 55.4 on activity; for diagnostic arthroscopy 31.4 at rest and 47.5 on activity). The observed mean difference between groups (ASD minus diagnostic arthroscopy) in pain VAS were -4.6 (95% confidence interval -11.3 to 2.1) points (P=0.18) at rest and -9.0 (-18.1 to 0.2) points (P=0.054) on arm activity. No between group differences were seen between the ASD and diagnostic arthroscopy groups in the secondary outcomes or adverse events. In the secondary comparison (ASD versus exercise therapy), statistically significant differences were found in favour of ASD in the two primary outcomes at 24 months in both VAS at rest (-7.5, -14.0 to -1.0, points; P=0.023) and VAS on arm activity (-12.0, -20.9 to -3.2, points; P=0.008), but the mean differences between groups did not exceed the pre-specified minimal clinically important difference. Of note, this ASD versus exercise therapy comparison is not only confounded by lack of blinding but also likely to be biased in favour of ASD owing to the selective removal of patients with likely poor outcome from the ASD group, without comparable exclusions from the exercise therapy group.
Conclusions: In this controlled trial involving patients with a shoulder impingement syndrome, arthroscopic subacromial decompression provided no benefit over diagnostic arthroscopy at 24 months.
Trial registration: Clinicaltrials.gov NCT00428870.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work other than those described above; ST reports personal fees from Evalua group of companies, personal fees from DBC group of companies, and personal fees from insurance companies, outside the submitted work; KK reports an honorarium for a lecture from Linvatec, outside the submitted work; TLNJ reports an honorarium for a lecture on osteoporosis from AMGEN (donated to AllTrials campaign); no other relationships or activities that could appear to have influenced the submitted work.
Figures


Comment in
-
In Shoulder Impingement Syndrome, Subacromial Decompression Did Not Differ from Diagnostic Arthroscopy for Shoulder Pain at 24 Months.J Bone Joint Surg Am. 2019 Feb 20;101(4):369. doi: 10.2106/JBJS.18.01342. J Bone Joint Surg Am. 2019. PMID: 30801377 No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical