

Heterogeneous expression of cytokines accounts for clinical diversity and refines prognostication in CMML
- PMID: 30026572
- PMCID: PMC7787307
- DOI: 10.1038/s41375-018-0203-0
Heterogeneous expression of cytokines accounts for clinical diversity and refines prognostication in CMML
Abstract
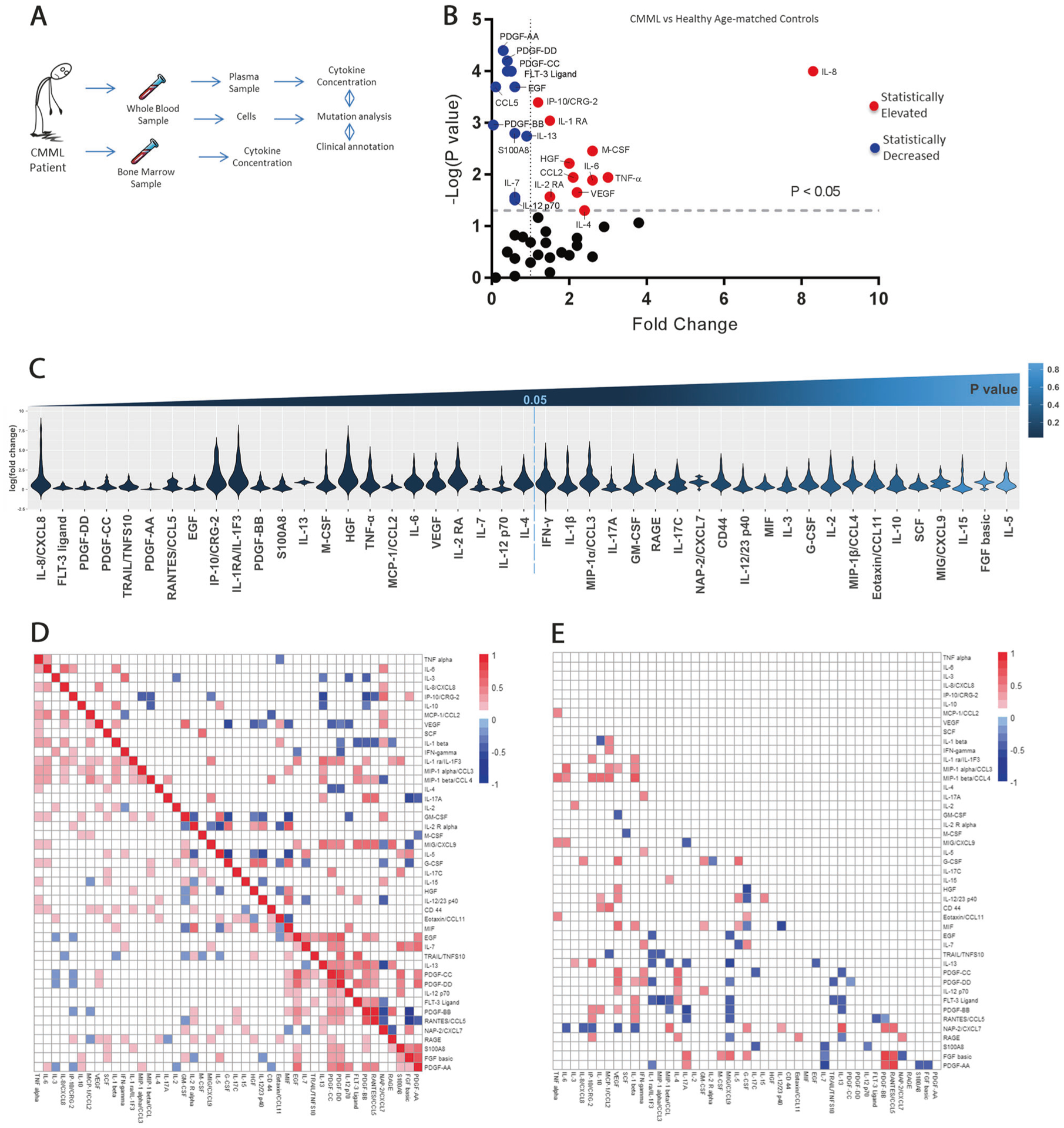
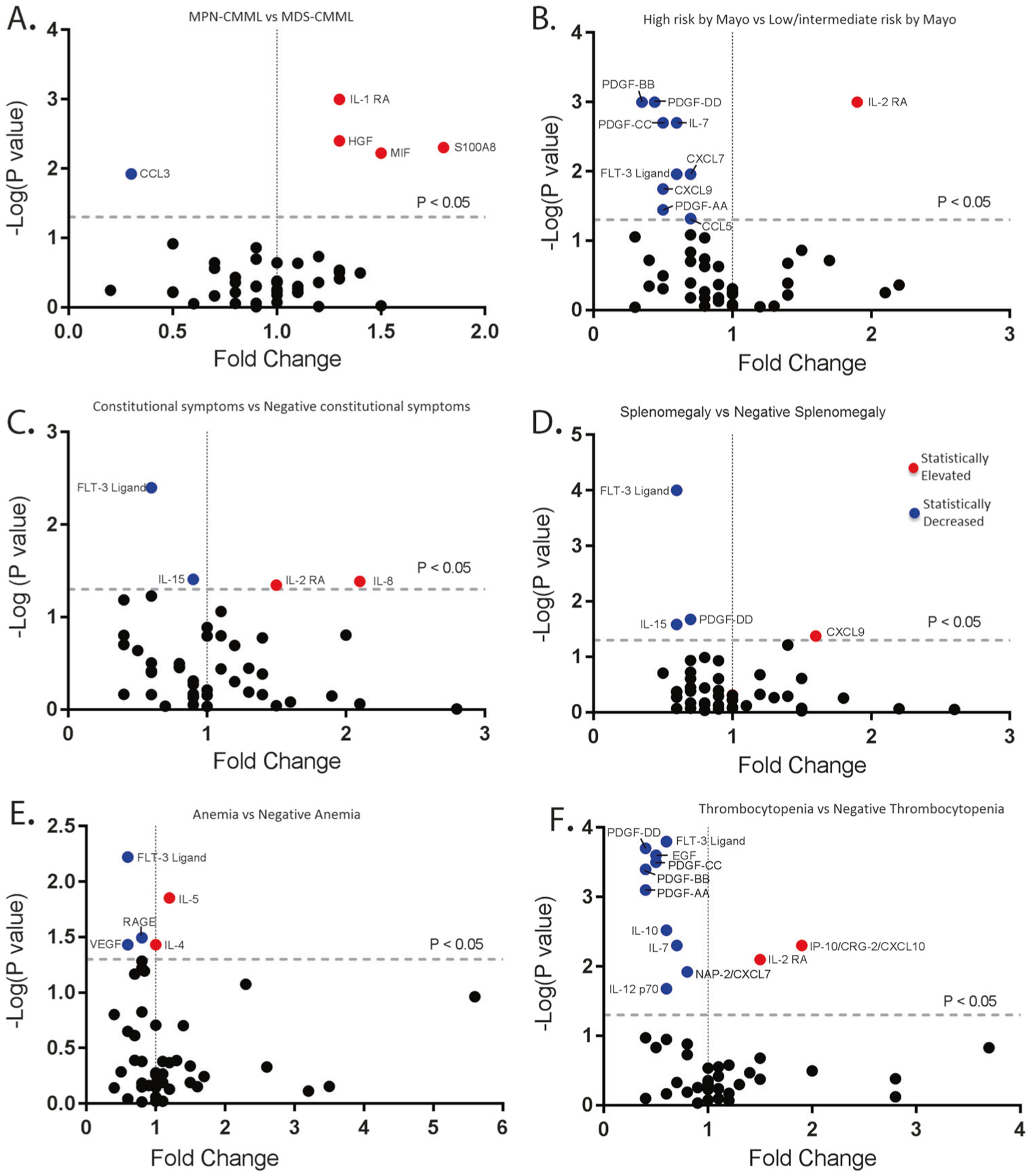
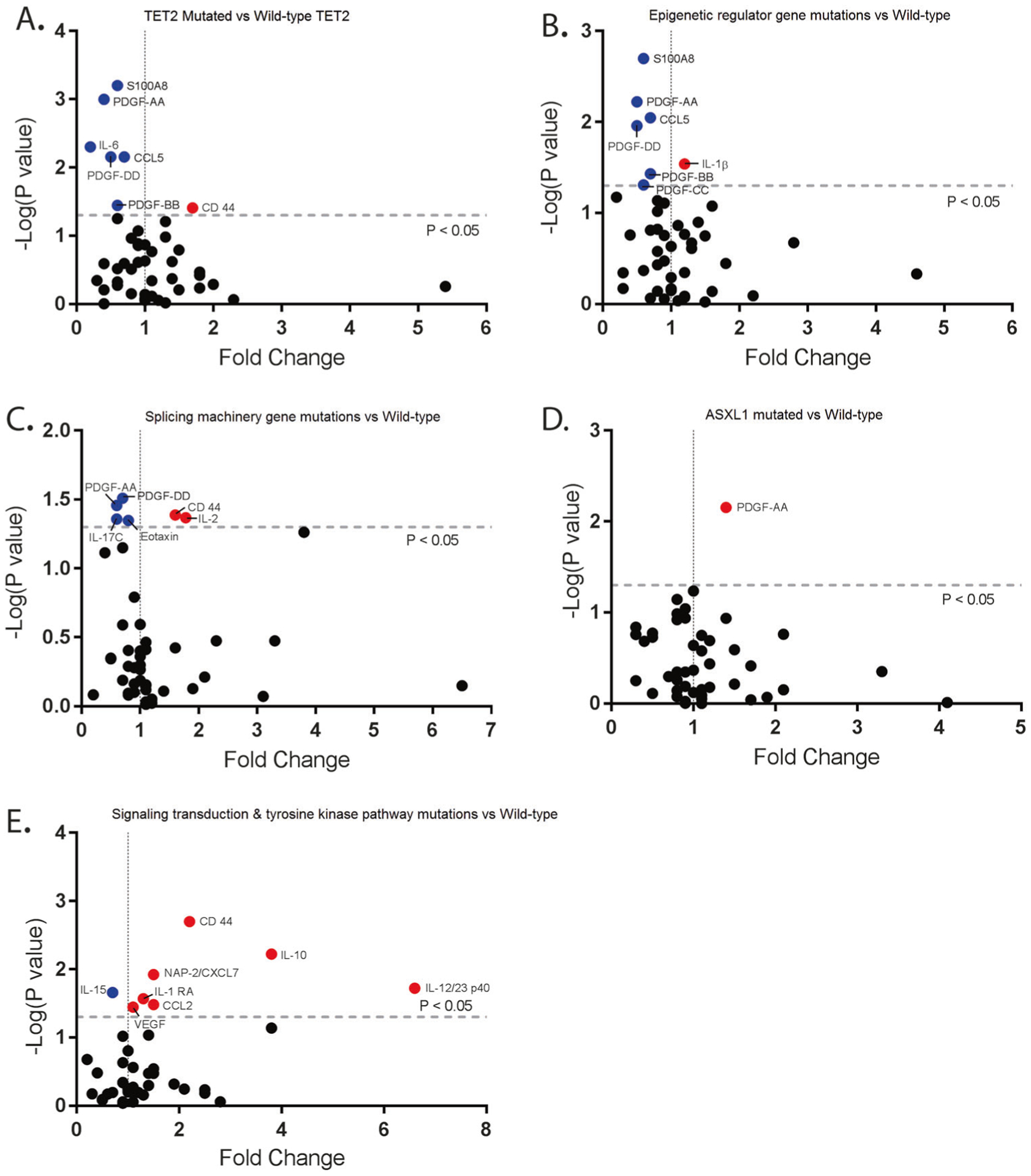
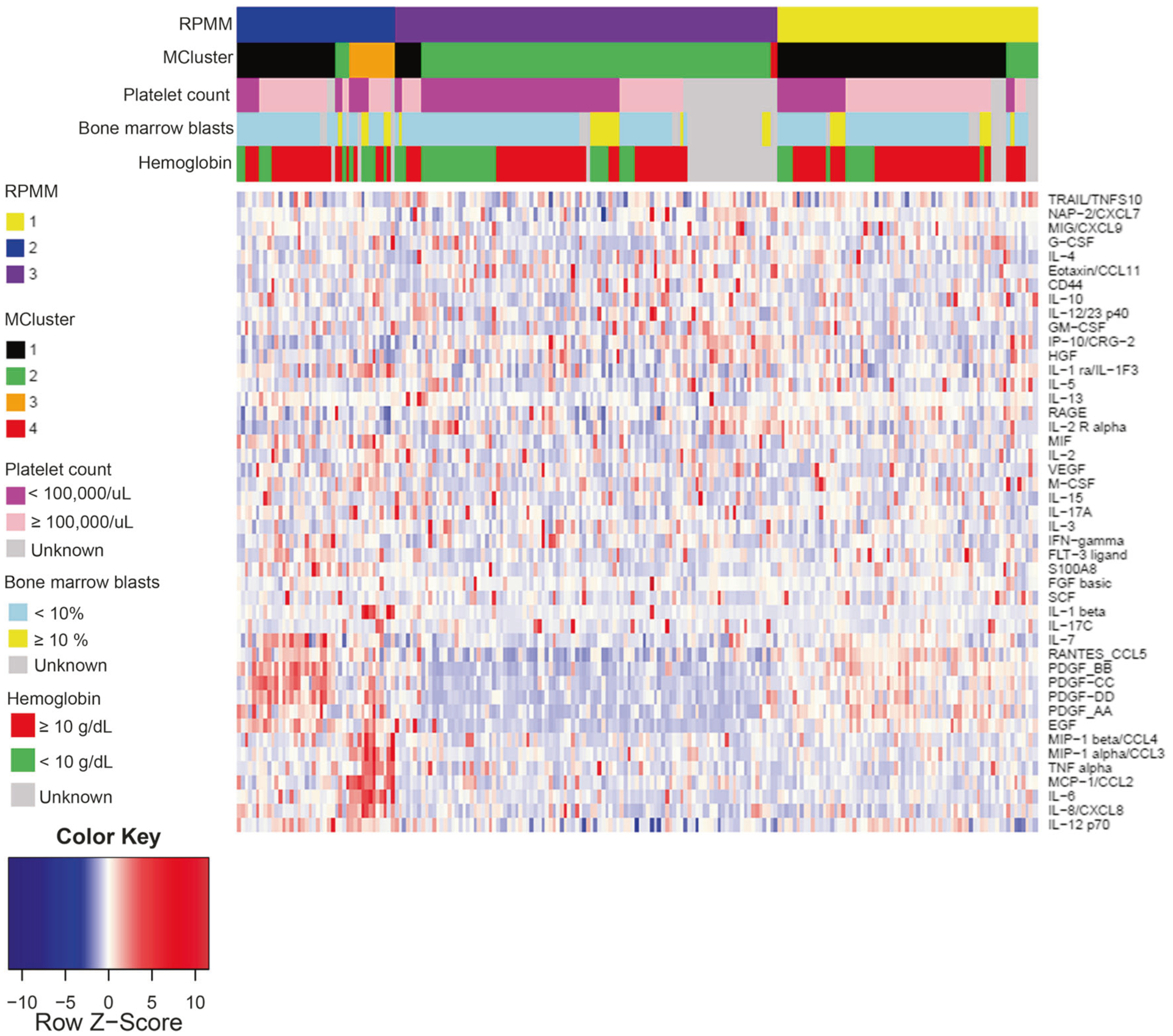
Chronic myelomonocytic leukemia (CMML) is a clinically heterogeneous neoplasm in which JAK2 inhibition has demonstrated reductions in inflammatory cytokines and promising clinical activity. We hypothesize that annotation of inflammatory cytokines may uncover mutation-independent cytokine subsets associated with novel CMML prognostic features. A Luminex cytokine profiling assay was utilized to profile cryopreserved peripheral blood plasma from 215 CMML cases from three academic centers, along with center-specific, age-matched plasma controls. Significant differences were observed between CMML patients and healthy controls in 23 out of 45 cytokines including increased cytokine levels in IL-8, IP-10, IL-1RA, TNF-α, IL-6, MCP-1/CCL2, hepatocyte growth factor (HGF), M-CSF, VEGF, IL-4, and IL-2RA. Cytokine associations were identified with clinical and genetic features, and Euclidian cluster analysis identified three distinct cluster groups associated with important clinical and genetic features in CMML. CMML patients with decreased IL-10 expression had a poor overall survival when compared to CMML patients with elevated expression of IL-10 (P = 0.017), even when adjusted for ASXL1 mutation and other prognostic features. Incorporating IL-10 with the Mayo Molecular Model statistically improved the prognostic ability of the model. These established cytokines, such as IL-10, as prognostically relevant and represent the first comprehensive study exploring the clinical implications of the CMML inflammatory state.
Conflict of interest statement
Figures
References
-
- Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, et al. The2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127:2391–405. - PubMed
-
- Bennett JM, Catovsky D, Daniel MT, Flandrin G, Galton DA, Gralnick HR, et al. Proposals for the classification of the acute leukaemias. French-American-British (FAB) co-operative group. Br J Haematol. 1976;33:451–8. - PubMed
-
- Ball M, List AF, Padron E. When clinical heterogeneity exceeds genetic heterogeneity: thinking outside the genomic box in chronic myelomonocytic leukemia. Blood. 2016;128:2381–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
