

Schmid's Type of Metaphyseal Chondrodysplasia: Diagnosis and Management
- PMID: 30027601
- PMCID: PMC6594483
- DOI: 10.1111/os.12382
Schmid's Type of Metaphyseal Chondrodysplasia: Diagnosis and Management
Abstract
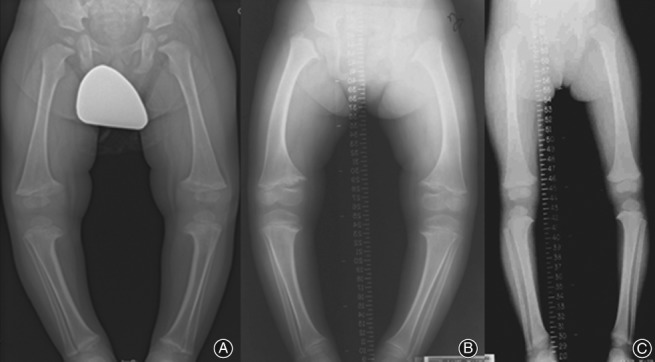
Objectives: There are several types of metaphyseal chondrodysplasia and various clinical types have been differentiated. The Schmid type of metaphyseal chondrodysplasia is the most common. Diffuse metaphyseal flaring, irregularity, and growth plate widening, which are most severe in the knees, are the most striking radiological features of this disease. The Schmid type of metaphyseal dysostosis is characterized by failure of normal mineralization of the zone of provisional calcification, leading to widened physes and enlarged knobby metaphyses, effectively causing shortening of the tubular bones, splaying of the metaphyses, coxa vara, and bow legs. Orthopaedic interventions were primarily performed on the lower extremities.
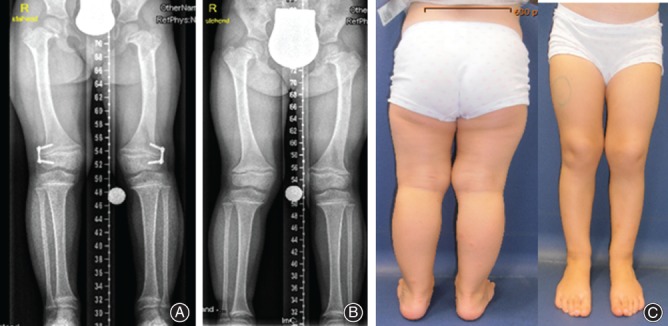
Methods: Twelve children (seven girls and five boys) aged 7-10 years were enrolled in this study. Moderate short stature was a uniform feature associated with predominant involvement of the proximal femora and bow legs resulted in the development of angular deformities. A waddling gait was a consequence of coxa vara in eight children. Valgus osteotomy of the proximal femur was planned after physeal closure for the group of children with coxa vara. Hemiepiphysiodesis was performed to re-align the genu varum in three children.
Results: Other forms of metaphyseal dysostosis were ruled based on full clinical and radiographic phenotypes, with confirmation through molecular pathology. Mutations in the COL10A1 gene located on chromosome 6q21-q22.3 were confirmed. Re-alignment was accomplished in our group of patients.
Conclusion: The most striking clinical features of Schmid metaphyseal chondrodysplasia which appear within the first 2-3 years of life are: moderate short limbs and short stature, a waddling gait, and increasing shortness of stature with age. The Schmid type of metaphyseal chondrodysplasia is a disorder that arises from defective type X collagen, which is typically found in the hypertrophic zone of the physes. Moderate short stature and a waddling gait associated with pain are the most common clinical presentations. Osteotomies to correct bow legs are sometimes combined with lengthening procedures. Recurrence of the deformities with growth is not uncommon; therefore, hemiepiphysiodesis or stapling might be indicated in some cases.
Keywords: Bowed legs; Metaphyseal dysostosis Schmid type; Mutations in the COL10A1; Surgical corrections.
© 2018 Chinese Orthopaedic Association and John Wiley & Sons Australia, Ltd.
Figures

References
-
- Schmid F. Beitrag zur Dysostosis enchondralis metaphysarea. Monats Kinderheilkd, 1949, 97: 393–397.
-
- Elliott AM, Field FM, Rimoin DL, Lachman RS. Hand involvement in Schmid metaphyseal chondrodysplasia. Am J Med Genet A, 2005, 132A: 191–193. - PubMed
-
- Stanley P, Sutcliffe J. Metaphyseal chondrodysplasia with dwarfism, pancreatic insufficiency and neutropenia. Pediatr Radiol, 1973, 1: 119–126. - PubMed
-
- Miller SM, Paul LW. Roentgen observations in familial metaphyseal dysostosis. Radiology, 1964, 83: 665–673. - PubMed
-
- Savarirayan R, Cormier‐Daire V, Lachman RS, Rimoin DL. Schmid type metaphyseal chondrodysplasia: a spondylometaphyseal dysplasia identical to the “Japanese” type. Pediatr Radiol, 2000, 30: 460–463. - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
