

Ultrasonography Findings in Severe Carpal Tunnel Syndrome
- PMID: 30027757
- PMCID: PMC6966291
- DOI: 10.1177/1558944718788642
Ultrasonography Findings in Severe Carpal Tunnel Syndrome
Abstract
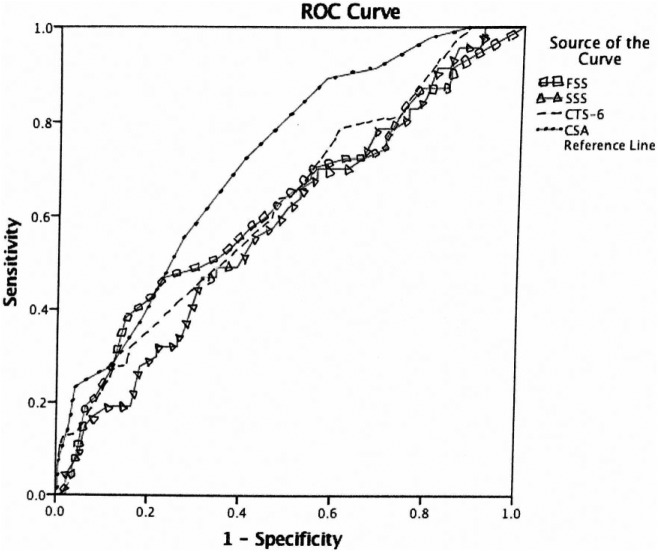
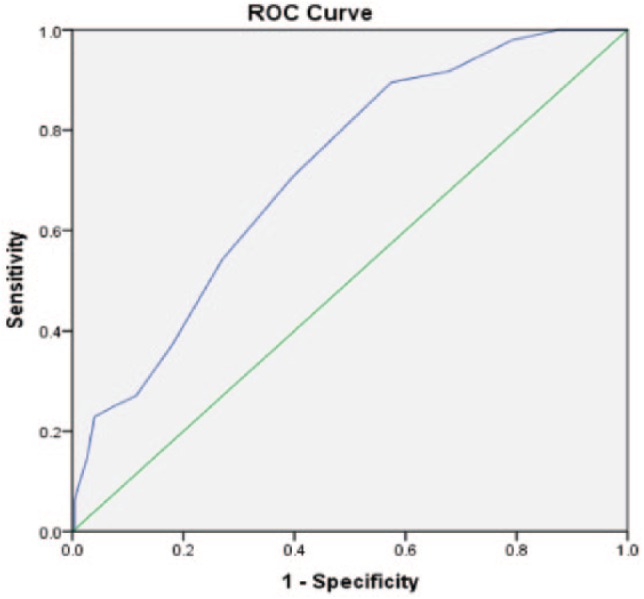
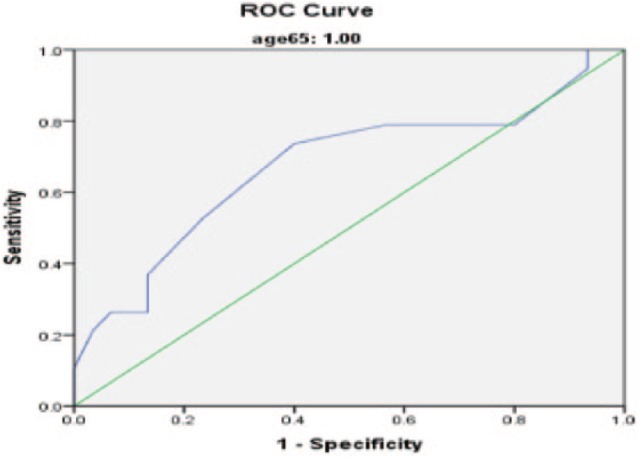
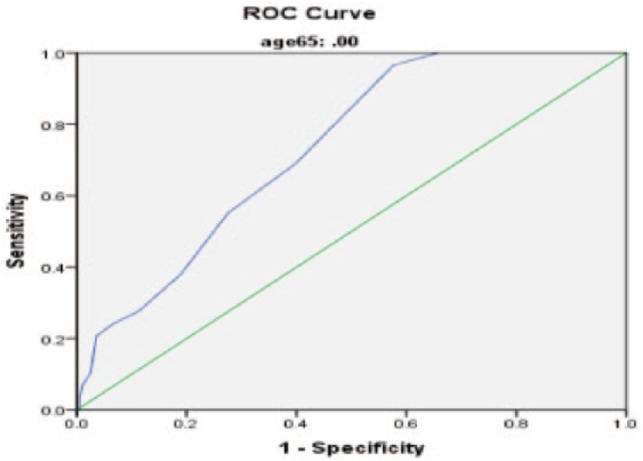
Background: Increasing severity of carpal tunnel syndrome (CTS), as graded by nerve conduction studies (NCS), has been demonstrated to predict the speed and completeness of recovery after carpal tunnel release (CTR). The purpose of this study is to compare the cross-sectional area (CSA) of the median nerve in patients with severe and nonsevere CTS as defined by NCS. Methods: Ultrasound CSA measurements were taken at the carpal tunnel inlet at the level of the pisiform bone by a hand fellowship-trained orthopedic surgeon. Severe CTS on NCS was defined as no response for the distal motor latency (DML) and/or distal sensory latency (DSL). Results: A total of 274 wrists were enrolled in the study. The median age was 51 years (range: 18-90 years), and 72.6% of wrists were from female patients. CSA of median nerve and age were comparatively the best predictors of severity using a linear regression model and receiver operator curves. Using cutoff of 12 mm2 for severe CTS, the sensitivity and specificity are 37.5% and 81.9%, respectively. Conclusions: Ultrasound can be used to grade severity in younger patients (<65 years) with a CTS-6 score of >12.
Keywords: carpal tunnel syndrome; measurement of the median nerve; median nerve cross-sectional area; nerve conduction studies; role of ultrasound in diagnosis; severity of carpal tunnel syndrome; test for severe carpal tunnel syndrome.
Conflict of interest statement
Figures
References
-
- Alfonso C, Jann S, Massa R, et al. Diagnosis, treatment and follow-up of the carpal tunnel syndrome: a review. Neurol Sci. 2010;31(3):243-252. - PubMed
-
- Chen YT, Williams L, Zak MJ, et al. Review of ultrasonography in the diagnosis of carpal tunnel syndrome and a proposed scanning protocol. J Ultrasound Med. 2016;35(11):2311-2324. - PubMed
-
- Fowler JR, Cipolli W, Hanson T. A comparison of three diagnostic tests for carpal tunnel syndrome using latent class analysis. J Bone Joint Surg Am. 2015;97(23):1958-1961. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
