

A Clinical Trial of TumorGlow to Identify Residual Disease During Pleurectomy and Decortication
- PMID: 30028985
- PMCID: PMC6296901
- DOI: 10.1016/j.athoracsur.2018.06.015
A Clinical Trial of TumorGlow to Identify Residual Disease During Pleurectomy and Decortication
Abstract
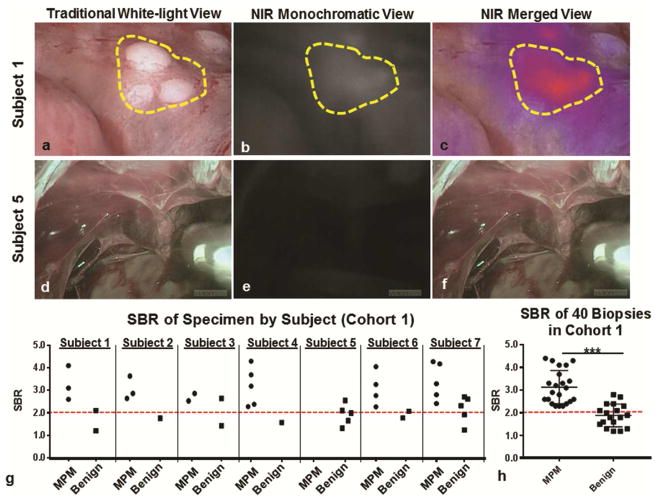
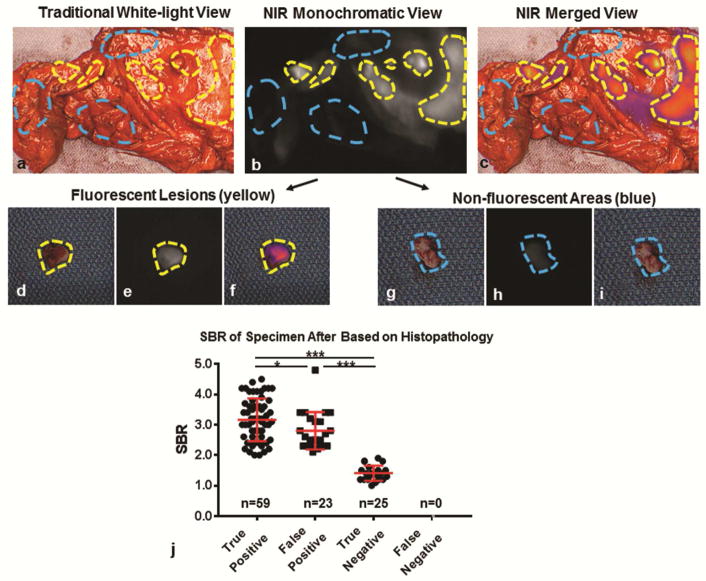
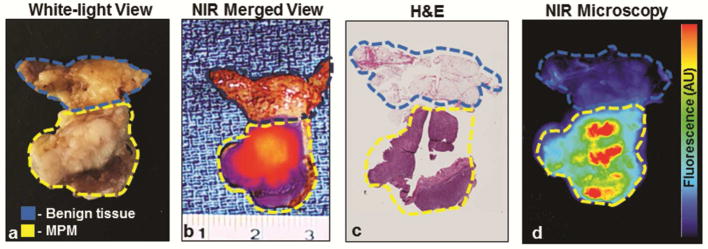
Background: Macroscopic complete resection can improve survival in a select group of patients with malignant pleural mesothelioma. During resection, differentiating residual tumor from inflammation or scar can be challenging. This trial evaluated near-infrared (NIR) intraoperative imaging using TumorGlow (a novel NIR imaging approach utilizing high-dose indocyanine green and delayed imaging) technology to improve detection of macroscopic residual disease.
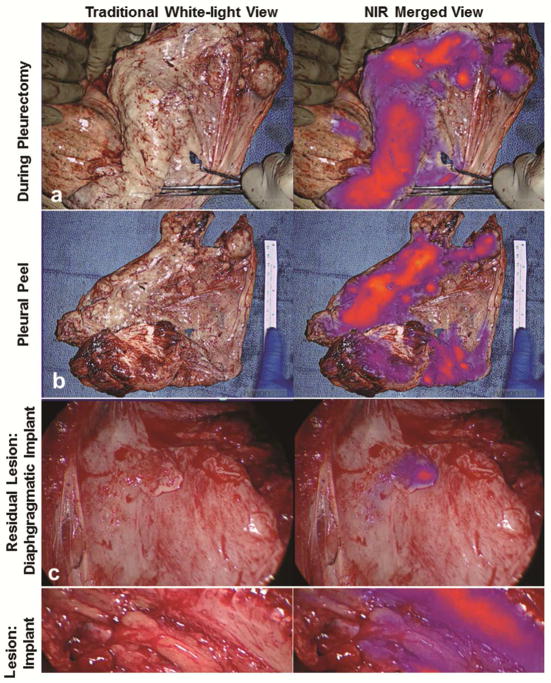
Methods: Twenty subjects were enrolled in an open-label clinical trial of NIR intraoperative imaging with TumorGlow (Indocyanine Green for Solid Tumors [NCT02280954]). Twenty-four hours before pleural biopsy or pleurectomy and decortication (P/D), patients received intravenous indocyanine green. All specimens identified during standard-of-care surgical resection and with NIR imaging underwent histopathologic profiling and correlative microscopic fluorescent tomographic evaluation. For subjects undergoing P/D (n = 13), the hemithorax was evaluated with NIR imaging during P/D to assess for residual disease. When possible, additional fluorescent lesions were resected.
Results: Of 203 resected specimens submitted for evaluation, indocyanine green accumulated within 113 of 113 of resected mesothelioma specimens, with a mean signal-to-background fluorescence ratio of 3.1 (SD, 2.2 to 4.8). The mean signal-to-background fluorescence ratio of benign tissues was 2.2 (SD, 1.4 to 2.4), which was significantly lower than in malignant specimens (p = 0.001). NIR imaging identified occult macroscopic residual disease in 10 of 13 subjects. A median of 5.6 resectable residual deposits per patient (range, 0 to 11 deposits per patient), with a mean size of 0.3 cm (range, 0.1 to 1.5 cm), were identified.
Conclusions: TumorGlow for malignant pleural mesothelioma is safe and feasible. Excellent sensitivity allows for to reliable detection of macroscopic residual disease during cytoreductive surgical procedures.
Copyright © 2019 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Wolf AS, Flores RM. Current treatment of mesothelioma: Extrapleural pneumonectomy versus pleurectomy/decortication. Thorac Surg Clin. 2016;26(3):359–375. - PubMed
-
- Vogelzang NJ, Rusthoven JJ, Symanowski J, et al. Phase iii study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J Clin Oncol. 2003;21(14):2636–2644. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
