

Current and Emerging Therapies in the Management of Hypoxic Ischemic Encephalopathy in Neonates
- PMID: 30029531
- PMCID: PMC6069156
- DOI: 10.3390/children5070099
Current and Emerging Therapies in the Management of Hypoxic Ischemic Encephalopathy in Neonates
Abstract
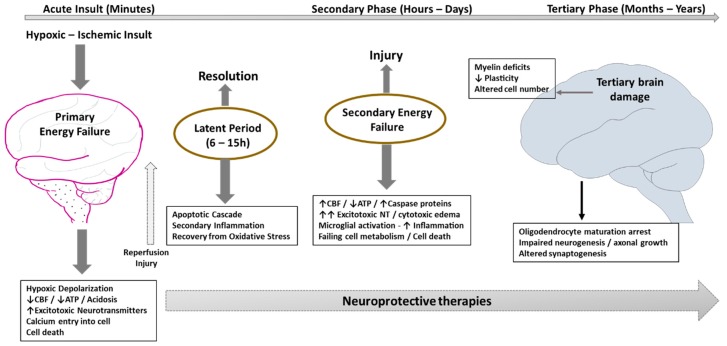
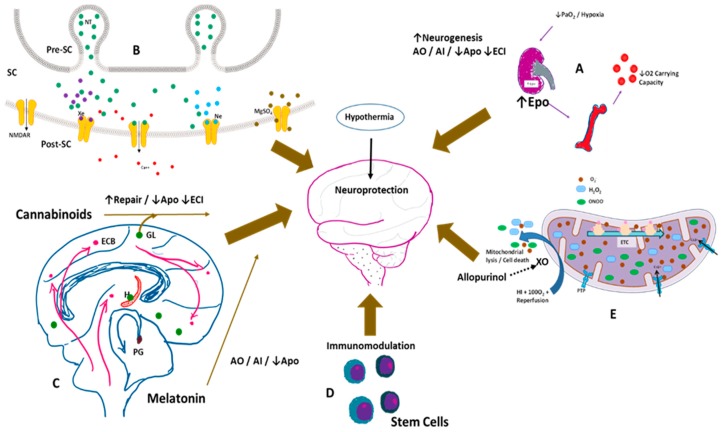
Neonatal hypoxic ischemic encephalopathy (HIE) presents a significant clinical burden with its high mortality and morbidity rates globally. Therapeutic hypothermia (TH) is now standard of care for infants with moderate to severe HIE, but has not definitively changed outcomes in severe HIE. In this review, we discuss newer promising markers that may help the clinician identify severity of HIE. Therapies that are beneficial and agents that hold promise for neuroprotection are described, both for use either alone or as adjuncts to TH. These include endogenous pathway modifiers such as erythropoietin and analogues, melatonin, and remote ischemic post conditioning. Stem cells have therapeutic potential in this condition, as in many other neonatal conditions. Of the agents listed, only erythropoietin and analogues are currently being evaluated in large randomized controlled trials (RCTs). Exogenous therapies such as argon and xenon, allopurinol, monosialogangliosides, and magnesium sulfate continue to be investigated. The recognition of tertiary mechanisms of brain damage has opened up new research into therapies not only to attenuate brain damage but also to promote cell repair and regeneration in a developmentally disorganized brain long after the perinatal insult. These alternative modalities may be especially important in mild HIE and in areas of the world where there is limited access to expensive hypothermia equipment and services.
Keywords: birth asphyxia; hypoxic ischemic encephalopathy; neonatal encephalopathy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Wyckoff M.H., Aziz K., Escobedo M.B., Kapadia V.S., Kattwinkel J., Perlman J.M., Simon W.M., Weiner G.M., Zaichkin J.G. Part 13: Neonatal resuscitation: 2015 american heart association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(Suppl. 2):S543–S560. doi: 10.1161/CIR.0000000000000267. - DOI - PubMed
-
- Shankaran S., Laptook A.R., Ehrenkranz R.A., Tyson J.E., McDonald S.A., Donovan E.F., Fanaroff A.A., Poole W.K., Wright L.L., Higgins R.D., et al. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N. Engl. J. Med. 2005;353:1574–1584. doi: 10.1056/NEJMcps050929. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
