

Challenges in Predicting Recurrence After Resection of Node-Negative Non-Small Cell Lung Cancer
- PMID: 30031845
- PMCID: PMC6347463
- DOI: 10.1016/j.athoracsur.2018.06.022
Challenges in Predicting Recurrence After Resection of Node-Negative Non-Small Cell Lung Cancer
Abstract
Background: One in 5 patients with completely resected early-stage non-small cell lung cancer will recur within 2 years. Risk stratification may facilitate a personalized approach to the use of adjuvant therapy and surveillance imaging. We developed a prediction model for recurrence based on five clinical variables (tumor size and grade, visceral pleural and lymphovascular invasion, and sublobar resection), and tested the hypothesis that the addition of several new molecular markers of poor long-term outcome (vascular endothelial growth factor C; microRNA precursors 486 and 30d) would enhance prediction.
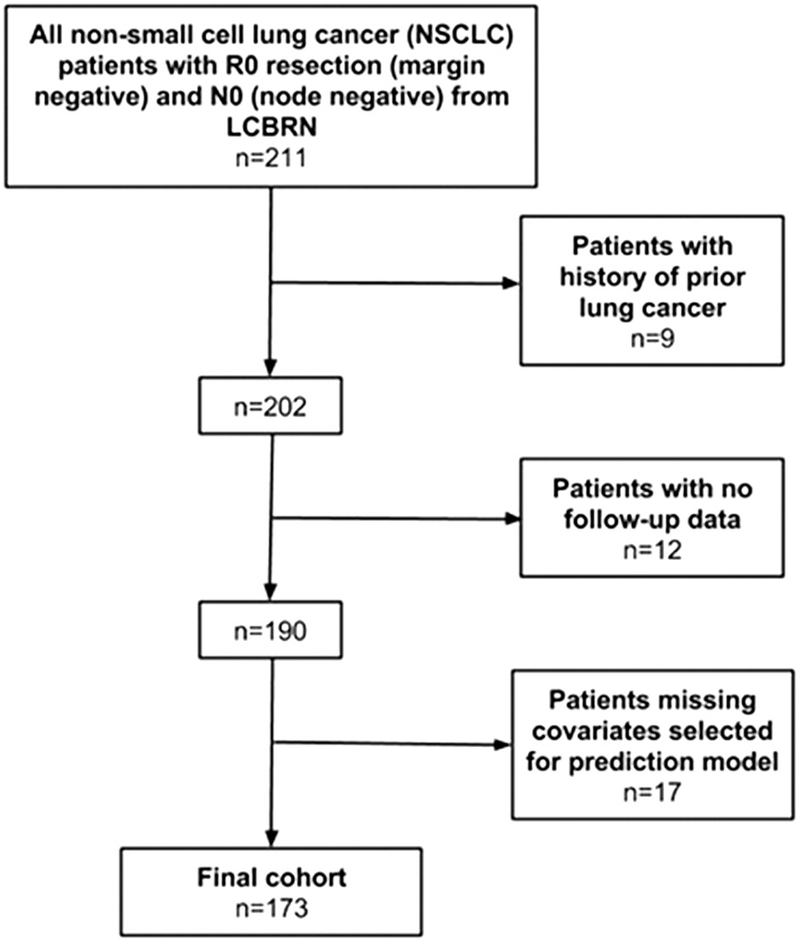
Methods: We performed a retrospective cohort study of patients with completely resected, node-negative non-small cell lung cancer from 2011 to 2014 (follow-up through 2016) using the Lung Cancer Biospecimen Resource Network. Cox regression was used to estimate the 2-year risk of recurrence. Our primary measure of model performance was the optimism-corrected C statistic.
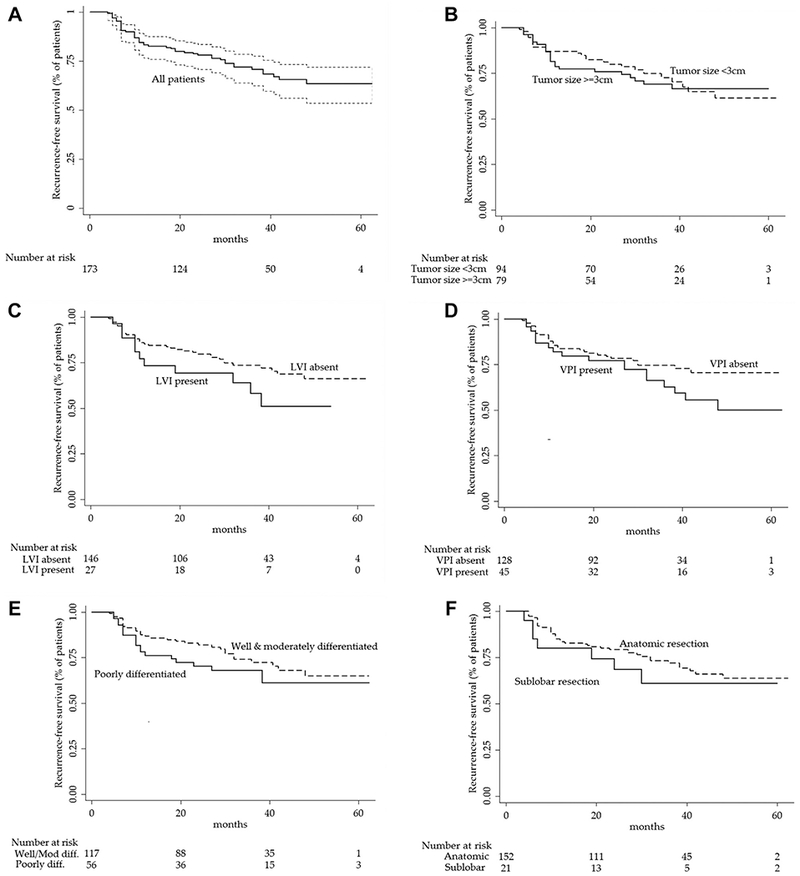
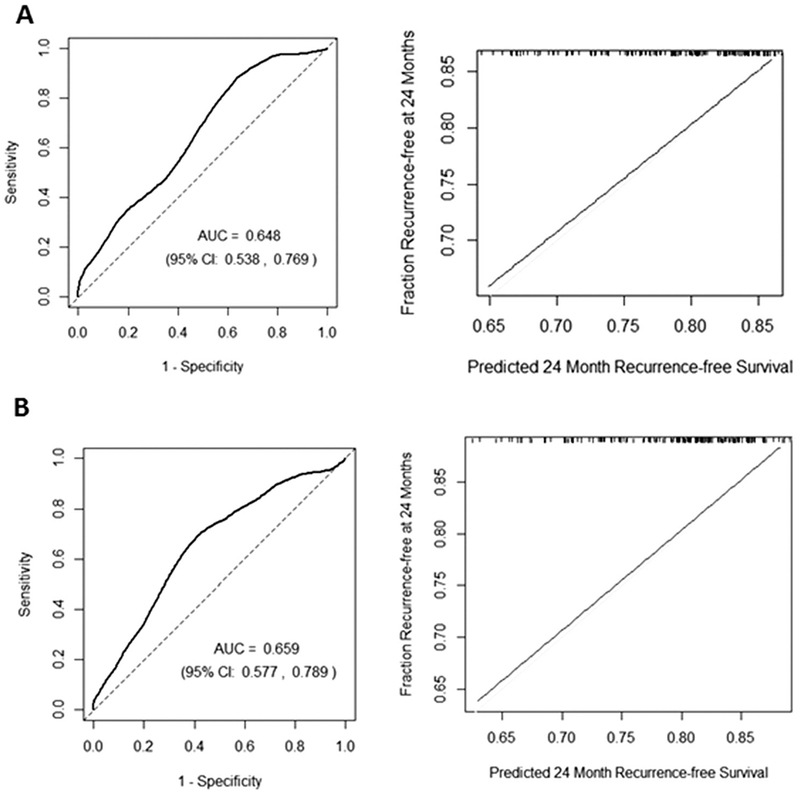
Results: Among 173 patients (mean tumor size, 3.6 cm; 12% sublobar resection, 32% poorly differentiated, 16% lymphovascular invasion, 26% visceral pleural invasion), the 2-year recurrence rate was 23% (95% confidence interval, 17% to 31%). A prediction model using five known risk factors for recurrence performed only slightly better than chance in predicting recurrence (optimism-corrected C statistic, 0.54; 95% confidence interval, 0.51 to 0.68). The addition of biomarkers did not improve the model's ability to predict recurrence (corrected C statistic, 0.55; 95% confidence interval, 0.52 to 0.71).
Conclusions: We were unable to predict lung cancer recurrence using a risk-prediction model based on five well-known clinical risk factors and several biomarkers. Further research should consider novel predictors of recurrence to stratify patients with completely resected early-stage non-small cell lung cancer according to their risk of recurrence.
Copyright © 2018 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Torre LA, Siegel RL, Jemal A. Lung Cancer Statistics. Adv Exp Med Biol 2016;893:1–19. - PubMed
-
- Little AG, Gay EG, Gaspar LE, Stewart AK. National survey of non-small cell lung cancer in the United States: epidemiology, pathology and patterns of care. Lung Cancer 2007;57:253–60. - PubMed
-
- Gould MK, Tang T, Liu ILA, et al. Recent trends in the identification of incidental pulmonary nodules. Am J Respir Crit Care Med 2015;192:1208–14. - PubMed
-
- Kiankhooy A, Taylor MD, LaPar DJ, et al. Predictors of early recurrence for node-negative T1 to T2b non-small cell lung cancer. Ann Thorac Surg 2014;98:1175–83. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
