

Manufacturing Mesenchymal Stromal Cells for the Treatment of Graft-versus-Host Disease: A Survey among Centers Affiliated with the European Society for Blood and Marrow Transplantation
- PMID: 30031938
- PMCID: PMC6299357
- DOI: 10.1016/j.bbmt.2018.07.015
Manufacturing Mesenchymal Stromal Cells for the Treatment of Graft-versus-Host Disease: A Survey among Centers Affiliated with the European Society for Blood and Marrow Transplantation
Abstract
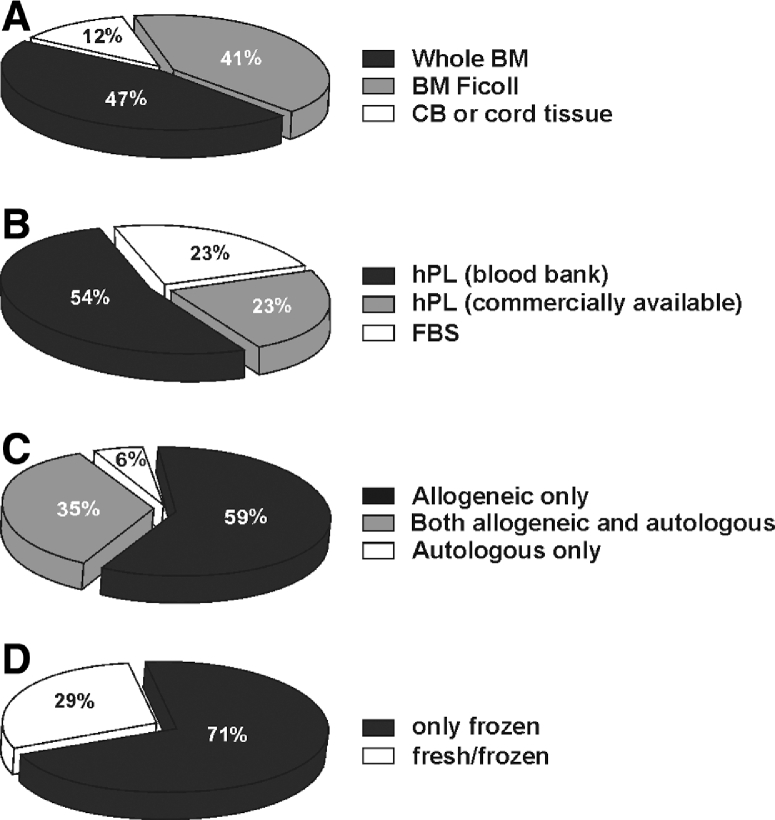
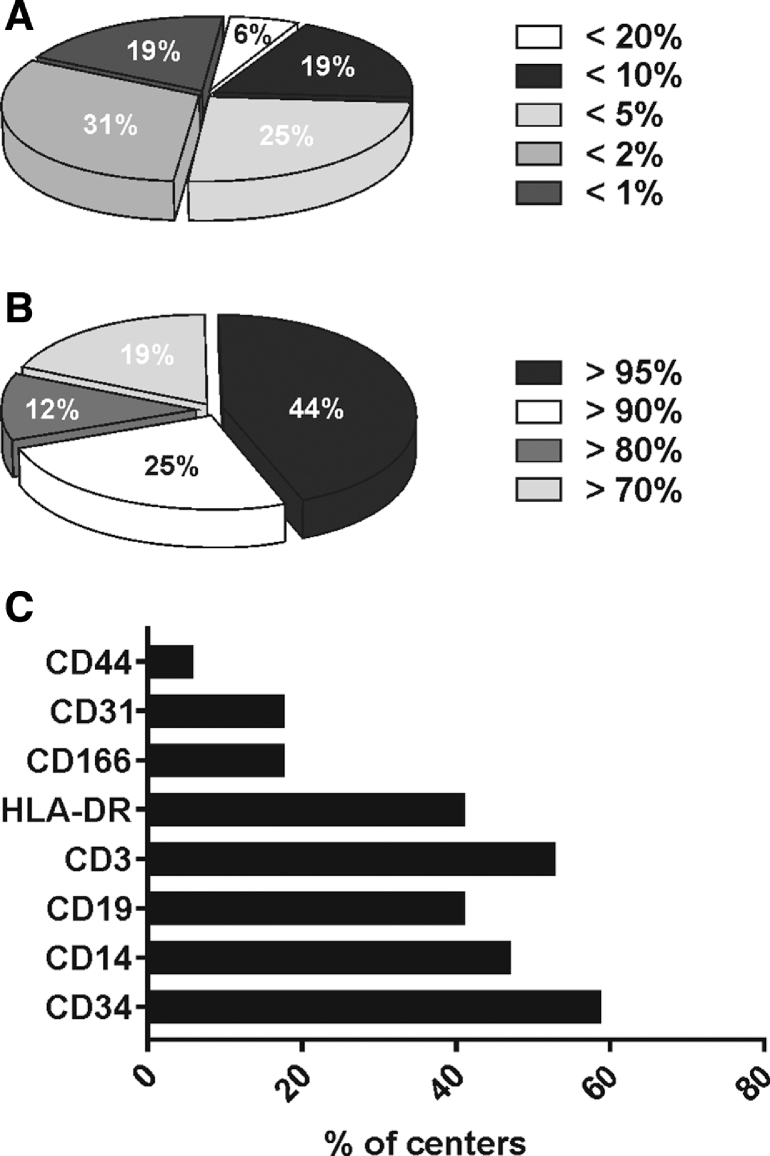
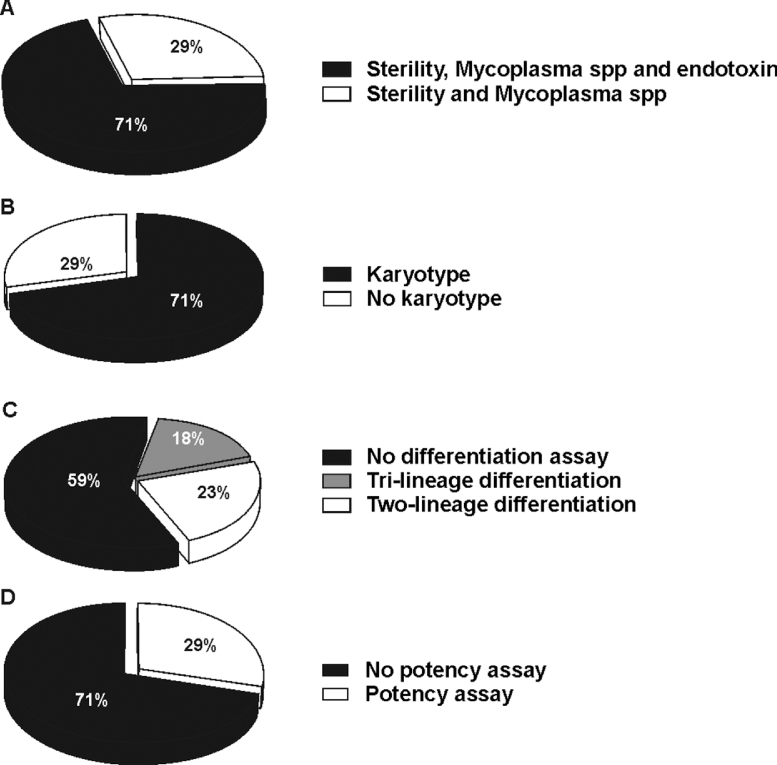
The immunosuppressive properties of mesenchymal stromal cells (MSC) have been successfully tested to control clinical severe graft-versus host disease and improve survival. However, clinical studies have not yet provided conclusive evidence of their efficacy largely because of lack of patients' stratification criteria. The heterogeneity of MSC preparations is also a major contributing factor, as manufacturing of therapeutic MSC is performed according to different protocols among different centers. Understanding the variability of the manufacturing protocol would allow a better comparison of the results obtained in the clinical setting among different centers. In order to acquire information on MSC manufacturing we sent a questionnaire to the European Society for Blood and Marrow Transplantation centers registered as producing MSC. Data from 17 centers were obtained and analyzed by means of a 2-phase questionnaire specifically focused on product manufacturing. Gathered information included MSC tissue sources, MSC donor matching, medium additives for ex vivo expansion, and data on MSC product specification for clinical release. The majority of centers manufactured MSC from bone marrow (88%), whilst only 2 centers produced MSC from umbilical cord blood or cord tissue. One of the major changes in the manufacturing process has been the replacement of fetal bovine serum with human platelet lysate as medium supplement. 59% of centers used only third-party MSC, whilst only 1 center manufactured exclusively autologous MSC. The large majority of these facilities (71%) administered MSC exclusively from frozen batches. Aside from variations in the culture method, we found large heterogeneity also regarding product specification, particularly in the markers used for phenotypical characterization and their threshold of expression, use of potency assays to test MSC functionality, and karyotyping. The initial data collected from this survey highlight the variability in MSC manufacturing as clinical products and the need for harmonization. Until more informative potency assays become available, a more homogeneous approach to cell production may at least reduce variability in clinical trials and improve interpretation of results.
Keywords: Cellular therapy; Graft-versus-host disease; Manufacturing; Mesenchymal stromal cells; Product specification; Release criteria.
Copyright © 2018. Published by Elsevier Inc.
Figures
References
-
- Dominici M, Le Blanc K, Mueller I. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy. 2006;8:315–317. - PubMed
-
- Lv F-J, Tuan RS, Cheung KMC, Leung VYL. Concise review: the surface markers and identity of human mesenchymal stem cells. Stem Cells. 2014;32:1408–1419. - PubMed
-
- Crisan M, Yap S, Casteilla L. A perivascular origin for mesenchymal stem cells in multiple human organs. Cell Stem Cell. 2008;3:301–313. - PubMed
-
- Kalluri R, Zeisberg M. Fibroblasts in cancer. Nat Rev Cancer. 2006;6:392–401. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
