

Perspective: Limiting Dependence on Nonrandomized Studies and Improving Randomized Trials in Human Nutrition Research: Why and How
- PMID: 30032218
- PMCID: PMC6054237
- DOI: 10.1093/advances/nmy014
Perspective: Limiting Dependence on Nonrandomized Studies and Improving Randomized Trials in Human Nutrition Research: Why and How
Abstract
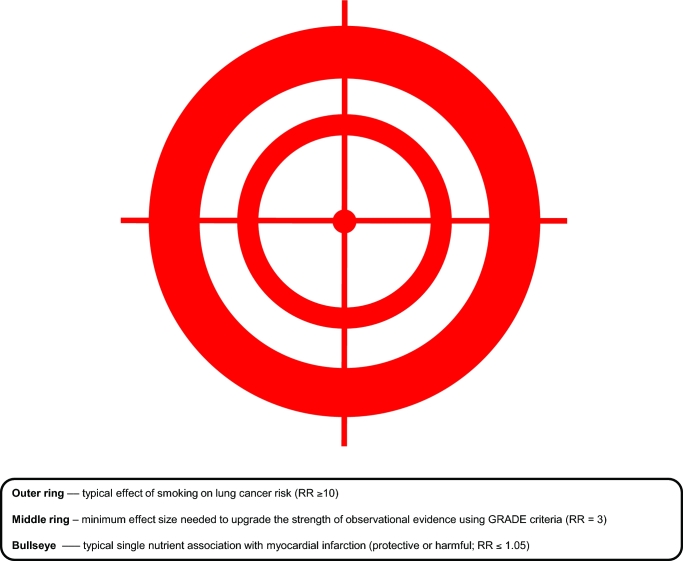
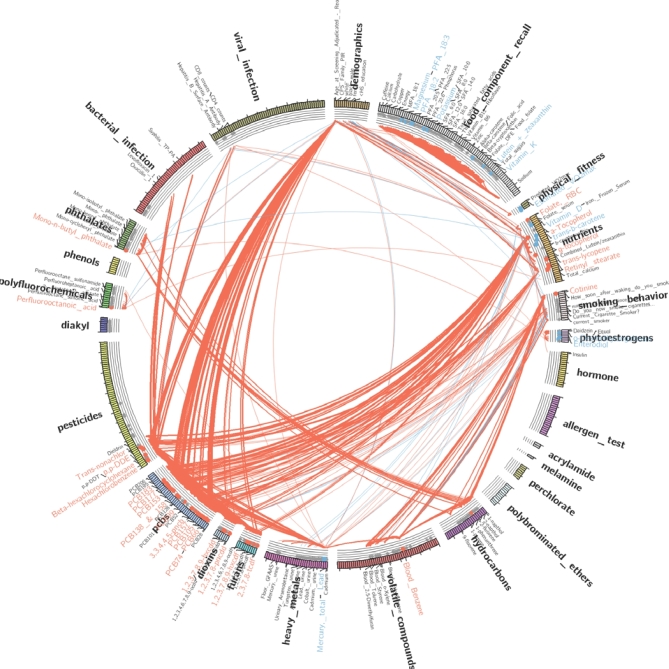
A large majority of human nutrition research uses nonrandomized observational designs, but this has led to little reliable progress. This is mostly due to many epistemologic problems, the most important of which are as follows: difficulty detecting small (or even tiny) effect sizes reliably for nutritional risk factors and nutrition-related interventions; difficulty properly accounting for massive confounding among many nutrients, clinical outcomes, and other variables; difficulty measuring diet accurately; and suboptimal research reporting. Tiny effect sizes and massive confounding are largely unfixable problems that narrowly confine the scenarios in which nonrandomized observational research is useful. Although nonrandomized studies and randomized trials have different priorities (assessment of long-term causality compared with assessment of treatment effects), the odds for obtaining reliable information with the former are limited. Randomized study designs should therefore largely replace nonrandomized studies in human nutrition research going forward. To achieve this, many of the limitations that have traditionally plagued most randomized trials in nutrition, such as small sample size, short length of follow-up, high cost, and selective reporting, among others, must be overcome. Pivotal megatrials with tens of thousands of participants and lifelong follow-up are possible in nutrition science with proper streamlining of operational costs. Fixable problems that have undermined observational research, such as dietary measurement error and selective reporting, need to be addressed in randomized trials. For focused questions in which dietary adherence is important to maximize, trials with direct observation of participants in experimental in-house settings may offer clean answers on short-term metabolic outcomes. Other study designs of randomized trials to consider in nutrition include registry-based designs and "N-of-1" designs. Mendelian randomization designs may also offer some more reliable leads for testing interventions in trials. Collectively, an improved randomized agenda may clarify many things in nutrition science that might never be answered credibly with nonrandomized observational designs.
Figures
References
-
- Trinquart L, Johns DM, Galea S. Why do we think we know what we know? A metaknowledge analysis of the salt controversy. Int J Epidemiol 2016;45(1):251–60. - PubMed
-
- Benziger CP, Roth GA, Moran AE. The Global Burden of Disease Study and the preventable burden of NCD. Glob Heart 2016;11(4):393–7. - PubMed
-
- Ioannidis JP. Contradicted and initially stronger effects in highly cited clinical research. JAMA 2005;294(2):218–28. - PubMed
-
- Young SS, Karr A. Deming, data and observational studies. Significance 2011;8(3):116–20.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
