

The effect of chloroquine dose and primaquine on Plasmodium vivax recurrence: a WorldWide Antimalarial Resistance Network systematic review and individual patient pooled meta-analysis
- PMID: 30033231
- PMCID: PMC6105624
- DOI: 10.1016/S1473-3099(18)30348-7
The effect of chloroquine dose and primaquine on Plasmodium vivax recurrence: a WorldWide Antimalarial Resistance Network systematic review and individual patient pooled meta-analysis
Abstract
Background: Chloroquine remains the mainstay of treatment for Plasmodium vivax malaria despite increasing reports of treatment failure. We did a systematic review and meta-analysis to investigate the effect of chloroquine dose and the addition of primaquine on the risk of recurrent vivax malaria across different settings.
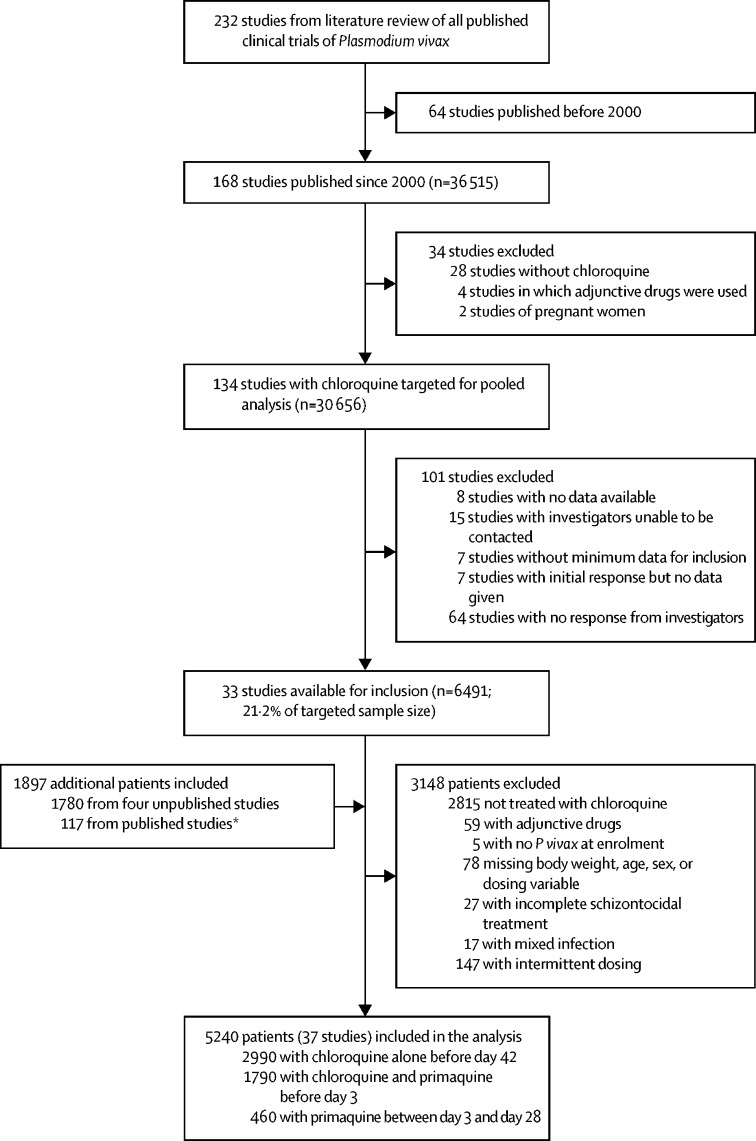
Methods: A systematic review done in MEDLINE, Web of Science, Embase, and Cochrane Database of Systematic Reviews identified P vivax clinical trials published between Jan 1, 2000, and March 22, 2017. Principal investigators were invited to share individual patient data, which were pooled using standardised methods. Cox regression analyses with random effects for study site were used to investigate the roles of chloroquine dose and primaquine use on rate of recurrence between day 7 and day 42 (primary outcome). The review protocol is registered in PROSPERO, number CRD42016053310.
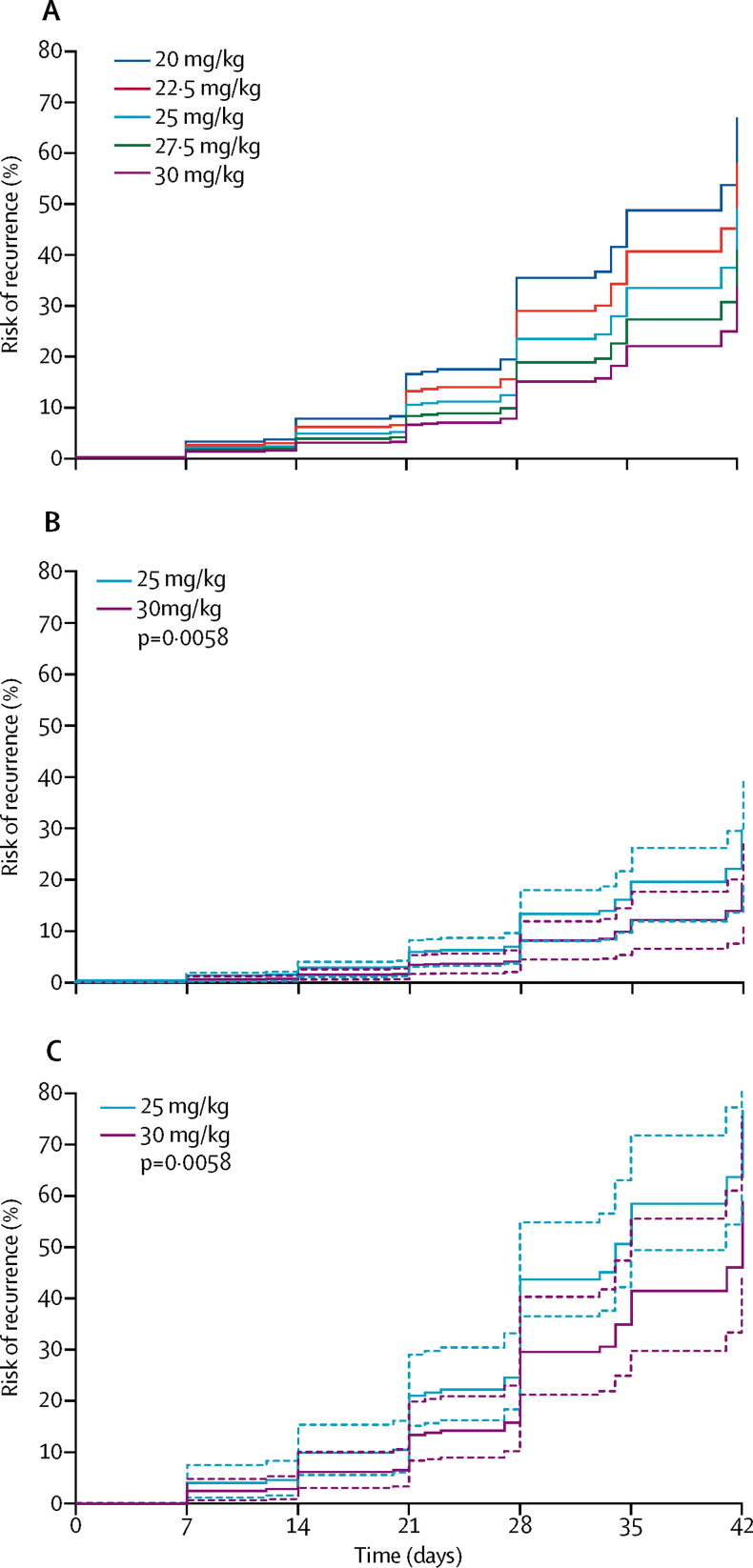
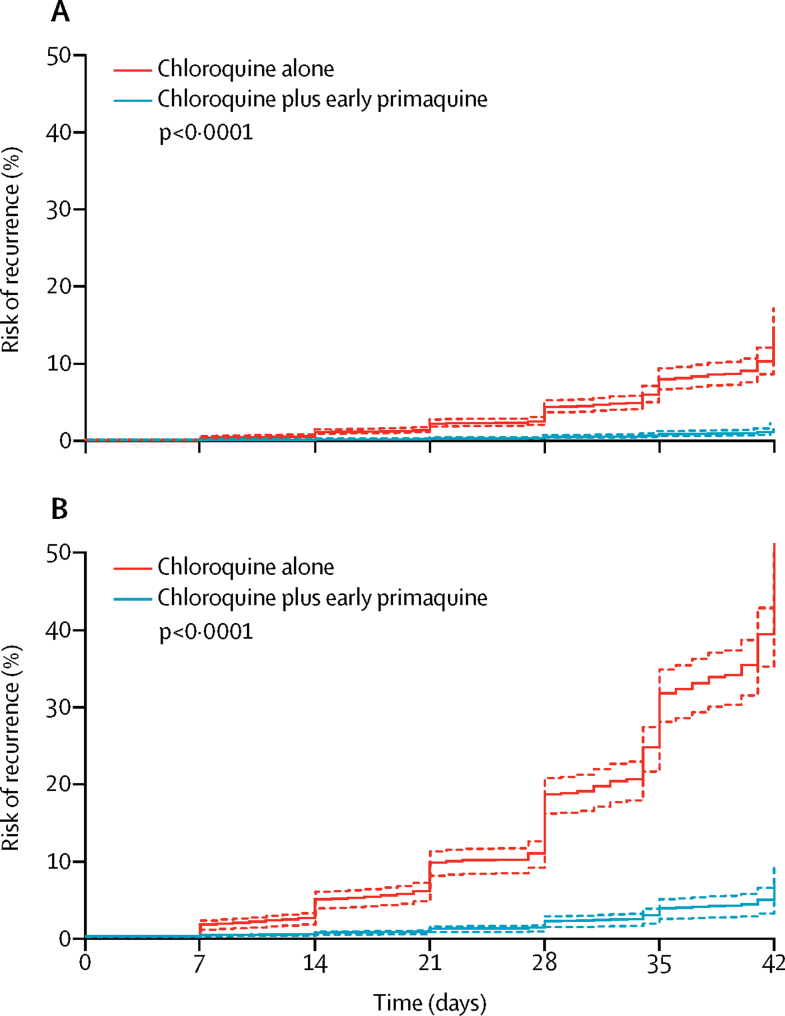
Findings: Of 134 identified chloroquine studies, 37 studies (from 17 countries) and 5240 patients were included. 2990 patients were treated with chloroquine alone, of whom 1041 (34·8%) received a dose below the target 25 mg/kg. The risk of recurrence was 32·4% (95% CI 29·8-35·1) by day 42. After controlling for confounders, a 5 mg/kg higher chloroquine dose reduced the rate of recurrence overall (adjusted hazard ratio [AHR] 0·82, 95% CI 0·69-0·97; p=0·021) and in children younger than 5 years (0·59, 0·41-0·86; p=0·0058). Adding primaquine reduced the risk of recurrence to 4·9% (95% CI 3·1-7·7) by day 42, which is lower than with chloroquine alone (AHR 0·10, 0·05-0·17; p<0·0001).
Interpretation: Chloroquine is commonly under-dosed in the treatment of vivax malaria. Increasing the recommended dose to 30 mg/kg in children younger than 5 years could reduce substantially the risk of early recurrence when primaquine is not given. Radical cure with primaquine was highly effective in preventing early recurrence and may also improve blood schizontocidal efficacy against chloroquine-resistant P vivax.
Funding: Wellcome Trust, Australian National Health and Medical Research Council, and Bill & Melinda Gates Foundation.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Improving Plasmodium vivax malaria treatment: a little more chloroquine.Lancet Infect Dis. 2018 Sep;18(9):934-935. doi: 10.1016/S1473-3099(18)30413-4. Epub 2018 Jul 20. Lancet Infect Dis. 2018. PMID: 30033232 No abstract available.
References
-
- Coatney GR. Pitfalls in a discovery: the chronicle of chloroquine. Am J Trop Med Hyg. 1963;12:121–128. - PubMed
-
- Rieckmann KH, Davis DR, Hutton DC. Plasmodium vivax resistance to chloroquine? Lancet. 1989;2:1183–1184. - PubMed
-
- Wellems TE, Plowe CV. Chloroquine-resistant malaria. J Infect Dis. 2001;184:770–776. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
