

The Interplay Between Keratinocytes and Immune Cells in the Pathogenesis of Psoriasis
- PMID: 30034395
- PMCID: PMC6043636
- DOI: 10.3389/fimmu.2018.01549
The Interplay Between Keratinocytes and Immune Cells in the Pathogenesis of Psoriasis
Abstract
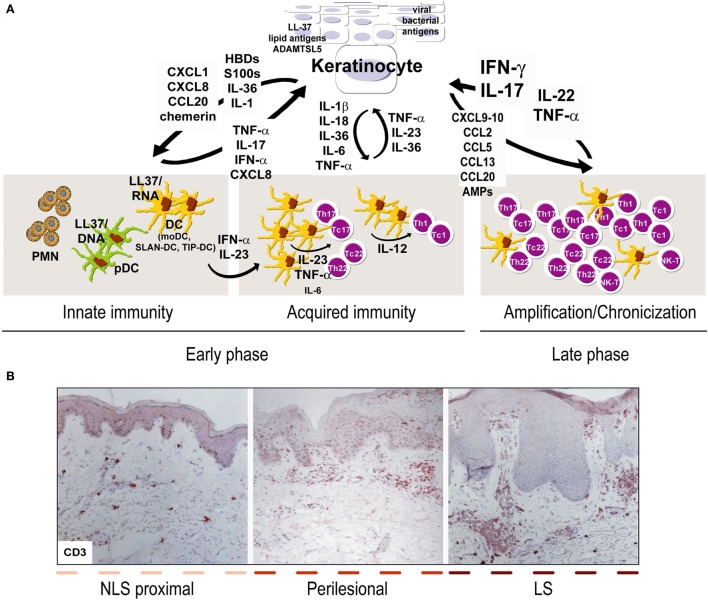
Psoriasis is a chronic inflammatory skin disease resulting from genetic, epigenetic, environmental, and lifestyle factors. To date, several immunopathogenic mechanisms of psoriasis have been elucidated, and, in the current model, the cross talk between autoreactive T cells and resident keratinocytes generates inflammatory and immune circuits responsible for the initiation, progression, and persistence of the disease. Several autoantigens derived from keratinocytes (i.e., LL37 cathelecidin/nucleic acid complexes, newly generated lipid antigens) have been identified, which may trigger initial activation of T cells, particularly IL-17-producing T cells, T helper (Th)1 and Th22 cells. Hence, lymphokines released in skin lesions are pivotal for keratinocyte activation and production of inflammatory molecules, which in turn lead to amplification of the local immune responses. Intrinsic genetic alterations of keratinocytes in the activation of signal transduction pathways dependent on T-cell-derived cytokines are also fundamental. The current review emphasizes the aberrant interplay of immune cells and skin-resident keratinocytes in establishing and sustaining inflammatory and immune responses in psoriasis.
Keywords: adaptive immunity; immune cells; innate immunity; keratinocytes; psoriasis; skin inflammation.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources